Dextromethorphan (DXM) is a dissociative with a more complex pharmacology than ketamine and PCP. In medicine it’s been used for cough, pain, pseudobulbar affect, and a variety of other conditions. It’s also a fairly common recreational drug.
The dose used for recreational effects ranges from 200 mg to more than 1,000 mg, with a common dose being around 250 to 600mg. Higher amounts can come with a higher rate of spiritual or interesting experiences, but the largest doses are riskier due to a higher rate of mania, confusion, and delusions. Although it’s a fairly safe substance in terms of physical effects even at ~1,000 mg, it’s best to remain in the common dose range for psychological safety.
Medical
Oral
For cough, DXM is given at 20-30 mg up to four times per day.
Itchiness (more common) and other allergic-like responses (rarer)
The effects can be compared to some aspects of simpler dissociatives and to the activity of psychedelics, but DXM does not fit neatly into any drug category. It has a wider array of effects than classic dissociatives due to its serotonergic properties, σ1 agonism, and other effects. Further, those effects change (as opposed to simply becoming more intense) as the dose increases.
It’s capable of eliciting euphoria, mild stimulation, mild hallucinations (such as slight visual distortions and depth perception impairment), and a general sense of intoxication that’s sometimes compared to ethanol beginning at 100 to 200 mg. It is not highly impairing at 100 to 200 mg, but it becomes very impairing at common+ doses.
We have a large number of reports on its recreational effects and those properties have also been investigated in studies, with people carefully being exposed to as much as 800 mg of DXM. High dose experiences can produce experiences that are similarly intense to psilocybin experiences, but with different qualitative content. Psychedelics are more likely to produce complex visual hallucinations and mystical experiences, although DXM does at least produce simple visual hallucinations and it can sometimes occasion out-of-body experiences, ego death, and other psychologically significant experiences.
Because of how intense and abnormal the experiences sometimes are, it can be difficult to retrospectively characterize them as “good” or “bad,” they’re just far from normal reality and sometimes distressing, meaningful, or entertaining.
Plateaus
Plateau 1: 1.5 to 2.5 mg/kg; 105 to 175 mg for a 70 kg person
Plateau 2: 2.5 to 7.5 mg/kg; 175 to 525 mg for a 70 kg person
Plateau 3: 7.5 to 15 mg/kg; 525 to 1,050 mg for a 70 kg person
Plateau 4: Over 15 mg/kg; ~Over 1050 mg for a 70 kg person
Plateau Sigma: Attained via redosing, typically with a total dosage equal to or greater than Plateau 4.
Likely in large part due to its complex pharmacology, both binding to various receptors and a change in the DXM:DXO ratio, there are benefits to viewing the effects through the lens of distinct groups. There are four well-characterized “plateaus” along with a fifth (Plateau Sigma) that some people experience with sufficient redosing. The simplest summary of these is that DXM’s recreational and euphoric effects are best experienced in Plateaus 1 (P1) and 2 (P2), while the hallucinogenic and spiritual effects are most notable at Plateau 3 (P3) and Plateau 4 (P4). It also shifts from somewhat stimulating and sensation enhancing/altering to more sedating and sensation blunting between P1/P2 and P3/P4.
This is not to say P2 experiences cannot be difficult or confusing or hallucinogenic, but the likelihood of panic, confusion, and delusional thinking is substantially lower at those doses. These plateaus are by no means strict boundaries; you can experience effects typically reserved for Plateau 3 while in the Plateau 2 dose range and vice versa, for example. Because the boundaries are not fixed between experiences and between people, it’s best to initially use low doses to gauge your sensitivity and to see which amount is best for you.
Rarely is there any benefit to a Plateau 4 experience, much as most people do not need to take 500 μg of LSD to experience the greatest benefit from the substance. Plateau 4 tends to leave people in a functionally anesthetized state, yet not unconscious, leaving them unable to do more than lie down and venture inward. Unfortunately this functional anesthetization sometimes doesn’t take hold and people are able to act out in response to hallucinations and delusions, which can be very dangerous. The hallucinations are more likely to be delirious in nature in both P4 and Plateau Sigma; you can be left seeing and believing things that have no basis in reality.
Mental
Dissociation is the central psychological effect of DXM. Particularly with common+ doses, the drug increasingly causes a user to feel like they’re detached from their body, surroundings, and mind. Sensory inputs decline and are impaired to the extent that people may not feel themselves breathing or they can feel like they’re no longer living. The most intense experiences occur in P3 and higher, at which point some people forget who they are, where they are, or even (more rarely) that a drug is the cause of what they’re feeling.
Pharmacologically, it affects key mechanisms underlying memory, cognition, and perception, such that instead of just altering those, high doses primarily cut you off from them. This can leave a user in a strange and rarely experienced state of being conscious yet not having the normal feeling of being alive because their senses are impaired and they may not identify with their body or thoughts.
Once you are sufficiently detached, you may end up feeling like your life has been an illusion, that you’re the only real person in existence, or that you’ve become nothing more than your thoughts or consciousness. Those feelings can be distressing and often contribute to panic. Panic is a pretty common response at higher doses. It can leave you feeling like you’re dying and an impending sense of doom may be present. Part of the problem is that it can be unnerving to feel like a stranger in your own mind and body, which then triggers progressively worse thoughts.
Although a lot of this description makes the experience sound unpleasant, the other side of being dissociated is that it can feel peaceful and calming, even to the point of euphoria. It often provides antidepressant and anxiolytic effects. Being freed from physical and mental stressors can be a liberating experience when it goes right. It’s also common for people to more strongly attach meaning to everything they experience under the influence and sometimes people become introspective, which can make an experience spiritually and personally meaningful, though some of those thoughts can be delusional.
An inability to understand time is common. At common/strong doses this can produce substantial time dilation which causes an experience to feel much longer than it really is, which is a negative effect if your experience is unpleasant.
Thinking becomes more random and tangential. At its worst, it can be delusional. There are many reports (most often with P3 and above) of users thinking they are being chased, that people are trying to hurt them, that they are in contact with gods or demons, or that they can read minds. Paranoid ideation is a real concern with higher doses.
Some people receive some entactogen-like effects, such as euphoria, caring about others, and a reduction in anger. This is most often seen with lower doses (P1 and low P2).
Memory and cognition impairment dose-dependently increase, eventually making it hard to multitask and making it risky to be in dangerous areas, such as near traffic. It can become hard to follow conversations. Response time is impaired even at lower doses and the accuracy of your memory declines as you take more. One study found that on average, the benzodiazepine triazolam impaired memory more than common recreational doses of DXM, but DXM still had a negative effect.
Sleep tends to be impaired even at low doses. The impact on energy is a bit hard to explain, with DXM offering both sedating and stimulant effects depending on the dose and person. At lower doses it’s often stimulating, which may facilitate creative work.
Music can be enhanced or negatively affected. The experience of listening to music may become deeper, more meaningful, and richer at low to common doses, while it’s also possible to become detached from sound and for music to be distorted in a negative manner, especially at higher doses.
Visuals
DXM does cause visuals, but they primarily involve an inaccurate perception of your surroundings rather than the complex and colorful hallucinations seen with psychedelics. Depth perception is affected, objects can appear larger or smaller, you may perceive things as slanted or bending, and there can be frequent changes in the size and shape of objects.
Vision splitting and double vision are common. DXM perception can be like taking a movie and turning it into a collection of rapidly displayed pictures; there’s a disconnect between each frame that becomes noticeable. Your vision also becomes lower quality, such as with blurriness.
It can be difficult to read or focus your vision, in part from shakiness that can at times be caused not just by altered perception but from a physical change in the movement of your eyes, known as nystagmus. Shakiness and focus impairment are dose-dependent.
Some color changes can occur, there can be light flashes, and some people report trailing beginning at low doses.
DXM can occasion more complex imaginative experiences, mostly when your eyes are closed and common or strong doses are used. Although the most reliable closed eye visuals are simple geometric hallucinations and colors, it can also produce out-of-body experiences, dream-like scenes, and “traveling” to new locations, environments, and situations. This becomes more likely as you become more disconnected from physical reality, so it’s dose-dependent.
Users have reported seeing random objects or people/beings. Sometimes the imaginative closed-eye experience is like going through a storyline, whether it’s fictitious (e.g. seeing your own funeral due to believing you’ve died) or reliving a memory.
Physical
Motor impairment is a very reliable effect. It initially makes fine coordination and precise movements harder, and as the dose increases it can even make walking a very difficult task. Robotic-like movements are common and when you are moving, there can be a disconnect between your consciousness and body such that it feels like you’re watching another person move.
Experiences differ for how your limbs feel. Sometimes they feel much heavier than usual and therefore difficult to move, but they can also feel lighter or like gravity itself has declined, which makes movement easier in some respects. The lighter feeling is more common with lower doses.
People can have a tingling sensation in their body and touching things may be more enjoyable than usual, but if enough is used, it’s more common to feel numb and disconnected from tactile sensations. Numbing of the tongue and mouth contributes to difficulty talking; you’re just not connected with your body enough for it to work properly at common+ doses. Even if thinking is not greatly impaired, which it often isn’t at low and common doses, you may have slurred speech and a general inability to verbally express what you’re thinking.
Nausea and vomiting are very common. DXM itself produces this with a high frequency, though it may be more common with syrups and other products that contain a variety of inactive or active ingredients.
Some users report feeling like they have a high fever and are burning up. This can occur just with DXM, but it might be more common with certain co-ingredients, such as products containing chlorpheniramine. Cold sweats and a general feeling of being ill are also possible. These effects may not be entirely perceptual, a number of reports mention observers noting how a user looks pale or very red. To reduce the chance of these effects, try to exclusively use DXM and stick to doses between Plateaus 1 and 3.
It’s pretty common for people to experience heart palpitations, which can go hand-in-hand with panic. It’s important to remember that DXM itself almost never affects cardiovascular activity to a lethal degree.
After Effects
The after effects vary between users and between experiences. Often it does produce an afterglow with depression and anxiety reduction, with users reporting they feel refreshed beginning the next day. This can occur even after very negative acute experiences. A study on the recreational effects of DXM found that it, like psychedelics, can produce lasting positive effects on spirituality, life satisfaction, and mood. Those positive effects may last weeks, months, or longer in some cases.
But instead of an afterglow, other users report an annoyingly persistent sense of dissociation and a general hangover feeling, usually for no more than few days.
Cognitive impairment sometimes occurs in the after effect period, so some users report slow thinking and brain fog. This is a greater concern when using the drug frequently.
(Carbonaro, 2017) – DXM at ~450 mg produces significant effects with a similar intensity to psilocybin, though with different qualitative effects.
20 participants completed the study. They had significant experience with psychedelics and dissociatives.
Doses: psilocybin (10, 20, and 30 mg/70 kg), and DXM (400 mg/70 kg), and placebo.
19/20 were extensive CYP2D6 metabolizers
Within-subject, crossover design.
Results
Time-course
At doses producing significant effects, they were generally significant by 2 hours, had maximal intensity at 2 to 4 hours, and were decreasing by 6 hours. DXM and psilocybin had similar timelines, but DXM produced greater and longer lasting effects on the Balance task (balancing on one foot with eyes closed).
BP, HR, and pupil diameter
DXM and all psilocybin doses significantly increased SBP, HR, and pupil diameter, but not DBP.
Circular Lights (hand-eye coordination) and Balance task (balancing on one foot with eyes closed)
Both drugs decreased performance on both tasks. Psilocybin generally produced dose-related effects and DXM produced significantly larger decreases on the Balance task vs. all psilocybin doses.
Peak monitor ratings
Both increased peak monitor ratings of overall drug effect, restlessness/fidgety, peace/harmony, joy/intense happiness, and nausea/vomiting.
The high psilocybin dose produced significantly greater effects than DXM on joy/intense happiness, while DXM produced a significantly greater effect on nausea/vomiting.
Psilocybin, but not DXM, produced a rise in yawning and tearing/crying vs. placebo.
There were no other significant effects of either psilocybin or DXM on the other monitor-rated dimensions.
Peak participant ratings of subjective effects and somatic symptoms
Both increased peak participant ratings. DXM was not significantly different from the high psilocybin dose, with the exception that psilocybin ratings were higher for visual effects and absorption when listening to music, while DXM was greater for lightheaded/dizzy.
Nausea/emesis during session
No participant vomited after 10 or 20 mg psilocybin. 2/20 vomited after 30 mg psilocybin.
11/20 vomited after 400 mg DXM.
Vomiting typically occurred more than 90 min after capsule administration, so it likely did not impact absorption significantly.
Participant-rated measures assessed 7 hours after drug administration
Ratings of drug effect intensity did not differ between DXM and high dose psilocybin, indicating the overall perceived strength of effect was similar.
Likewise, DXM did not differ from high dose psilocybin on measures of impaired cognition and control, anxiety, elementary imagery, audiovisual synthesthesia, and the total score and most of the subscales on the Challenging Experience Questionnaire.
The 30 mg psilocybin dose (and often the 20 mg dose) produced significantly greater effects than DXM on 6/11 subscales of the 5D-ASC questionnaire, 4/6 subscales of the HRS, and the total score and most of the subscales on the Mystical Experience Questionnaire.
Notably, DXM produced significantly higher scores on the Disembodiment Scale of the 5D-ASC vs. each psilocybin dose.
Mystical experiences
Complete mystical experiences occurred in 0% of placebo, 0% of 10 mg psilocybin, 20% of 20 mg psilocybin, 40% of 30 mg psilocybin, and 0% of DXM experiences.
The incidence of complete mystical experience from 30 mg psilocybin is significantly greater vs. the incidence from DXM.
Visuals
Both increased a range of diverse visual effects. But of the 18 measures of visual effects, the high psilocybin dose produced significantly greater effects than DXM on 12/18, indicating greater movement and more frequent, brighter, distinctive, and complex (including textured and kaleidoscopic) images and visions.
With eyes open, psilocybin also produced greater visual effects than DXM.
The differences between drugs are consistent with vivid, complex, patterned, and colorful imagery after psilocybin and other tryptamine hallucinogens relative to ketamine, which leads to more dreamlike and less vivid visual imagery.
Music
Both increased the measures of absorption in and significance of music. But the high psilocybin dose produced a significantly greater effect on both.
Pharmacological Class Questionnaire
Placebo
70% rated it as most like placebo, 25% rated it as sedative-hypnotic/muscle relaxant/anxiolytic, and 5% selected MDMA.
Psilocybin
85% picked classical hallucinogen after 10 mg, 80% after 20 mg, and 90% after 30 mg.
Rated as 75% similar to classic hallucinogens at 10 mg, 83% similar at 20 mg, and 90% similar at 30 mg.
DXM
60% picked dissociative anesthetic. 10% picked hallucinogen, 10% picked MDMA, and 5% selected sedative-hypnotic/muscle relaxant/anxiolytic, and 15% indicated they did not know which class.
65% similar to the dissociative class, 28% similar to the classic hallucinogen class, and 27% similar to the unidentified “other” class
COI: Dr. Carbonaro is an employee of the U.S. Food and Drug Administration (FDA); however, the views presented in this article do not necessarily reflect those of the FDA and no official support or endorsement of this article by the FDA is intended or should be inferred. Roland Griffiths is on the Board of Directors of the Heffter Research Institute.
(Perry, 2015) – DXM is not highly impairing at 120 mg
40 participants. They received DXM 120 mg or guaifenesin 400 mg (active placebo). They received one of the drugs and then the other 24 hours later.
Results
There were no significant differences in the failure rates for the HGN (horizontal gaze nystagmus), WAT (walk and turn), OLS (one leg stand), or combined SFST (standardized field sobriety test).
There were no significant differences in the number of collisions during a driving simulator.
COI: Not reported
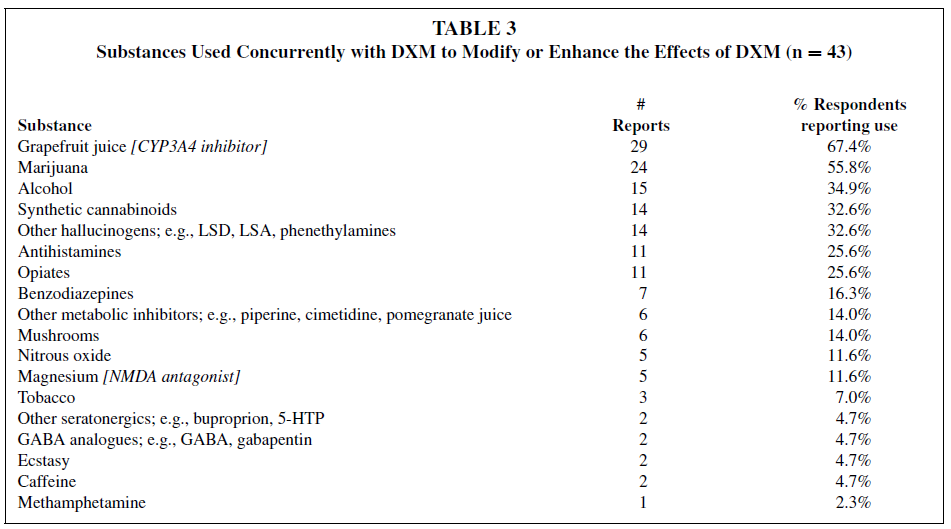
(Pringle, 2015) – Survey results from DXM users
60 individuals recruited from Dextroverse.org to discuss DXM. Mean age: 23.6
Results
Mean age at time of first DXM use: 17.1 years old
Mean lifetime DXM use: 150 times
Mean past-year use: 36 times
35/60 reported using it in the past month, with a mean of 4.8 times
General characteristics
Most first heard about it via the internet or a friend. They preferred to use DXM alone and they had not been in the hospital or police custody due to their use.
The tended to perceive it as safe, not widely known about, and in need of no greater restrictions.
82.7% reported taking other substances to modify or enhance the effects. And 34/43 listed more than one substance.
About two-thirds reported using grapefruit juice and over half used cannabis.
Intake of alcohol, synthetic cannabinoids, antihistamines, prescription opioids, and benzodiazepines was frequently noted.
COI: Not reported
(Carter, 2013 — using data from Reissig, 2012) – Evaluation of DXM’s cognitive effects at recreational doses
12 volunteers. They received placebo, triazolam, and DXM.
Triazolam was given at 0.25 and 0.5 mg/70 kg
DXM was given at up to 100, 200, 300, 400, 500, 600, 700, and 800 mg/70 kg.
The highest dose administered varied between participants. 2 received 400 mg, 2 received 500 mg, 4 received 600 mg, 2 received 700 mg, and 2 received 800 mg
Results
Digit-Symbol Substitution Test
Higher doses of both drugs (0.5 mg triazolam and 300 mg DXM) significantly decreased the number of trials attempted.
Divided Attention
Significant effects were seen at the low and high doses in the monitoring component of the task (proportion of targets correctly identified).
Only the high dose significantly affected the tracking component (tracking; deviation; distance in pixels between the diamond stimulus and cross hair)
The 100-300 mg/kg DXM doses were not significantly different from placebo for tracking, and the magnitude of effects were less than 0.5 mg triazolam on both parts of the test.
The penultimate (second highest for an individual) dose of DXM did significantly impair performance on both parts and did so similarly to triazolam 0.5 mg.
Working Memory
Significant effects of dose were observed for accuracy and response time.
Only the penultimate DXM dose led to a significant decline in accuracy compared to placebo. Whereas both doses of triazolam, 300 mg DXM, and the penultimate dose of DXM significantly increased median response times on the task.
Episodic Memory
The number of words correctly recalled was significantly decreased by both triazolam doses and by 100, 200, 300, and the penultimate DXM dose. However, the triazolam doses appeared to have a greater amnestic effect vs. the doses of DXM.
The mean number of words recalled after the penultimate DXM dose was the same as the number from 0.25 mg triazolam
Significant effects were also seen on the ability to correctly recognize a word as “new” or “old” (i.e. if they had previously seen it)
All conditions except for DXM 100 mg significantly decreased the discriminate index and again the triazolam doses were more anestic.
Both doses of triazolam and the penultimate dose of DXM, but not the lower 100/200/300 mg DXM doses, significantly decreased the hit rate (correctly recognizing a word as old) and false alarm rate (believing it was old but it’s actually new)
Metacognition
Participants’ estimate of the their DSST performance was not significantly affected.
In contrast, estimates of performance on the working memory task was significantly affected by both 0.5 mg triazolam and doses over 200 mg DXM.
COI: Funded by NIDA
(Reissig, 2012) – High DXM doses can produce classic hallucinogen-like effects
12 volunteers with a history of hallucinogen use, including classic psychedelics and often DXM (7/12). 3/12 had used PCP or ketamine.
All received placebo, two triazolam doses (0.25 and 0.5 mg/70 kg oral), and at least four doses of DXM (100, 200, 300, and 400 mg/70 kg oral). The highest dose administered was 400 mg/70 kg (n=2), 500 mg/70 kg (n=2), 600 mg/70 kg (n=4), 700 mg/70 kg (n=2), and 800 mg/70 kg (n=2).
Results
Time-course of drug effects
At doses producing significant effects, they were generally significant by 2 hours, at max from 2 to 4 hours, and declining by 6 hours.
Peak effects on measures assessed repeatedly during the session
BP and HR
DXM
Orderly and significant dose-related increases in SBP and DBP (20.8 and 14.6 mmHg, respectively).
Heart rate was significantly increased at the two highest DXM doses, by 26 at the max dose.
Triazolam
Small but significant decreases in SBP with no significant effect on DBP.
Heart was significantly increased by 10.2 at the 0.5 mg/70 kg dose.
Monitor ratings
DXM but not triazolam produced significant and dose-related increases on monitor ratings of distance from ordinary reality, visual effects with eyes open, visual effects with eyes closed, restlessness/fidgety, joy/euphoria/peace, nausea/vomiting, psychological discomfort, unresponsive to questions, anxiety or fearfulness, and confusion/disorientation. Triazolam but not DXM produced significant increases in sedation.
Neither drug significantly increased monitor ratings of stimulation/arousal, tearing/crying, or ideas of reference/paranoid thinking.
Participant ratings of subjective effects
DXM but not triazolam increased ratings of arousing/stimulating, lightheaded/dizzy, shaky/jittery, numbness/tingling, nervous/anxious, queasy/sick to stomach, hot-flushed, restless, talkative, limp/loose, headache, like drug effect, and dislike drug effect.
In contrast, triazolam, but not DXM, increased ratings of sleepy and tired/lazy and decreased ratings of energetic and excited.
Emesis
No volunteer vomited after receiving placebo, 0.25 or 0.5 mg/70 kg triazolam, or 100 or 200 mg/70 kg DXM. Two of the 12 volunteers vomited after receiving 300 mg/ 70 kg DXM. Seven of the 12 volunteers vomited after receiving a dose of 400 mg/70 kg DXM or greater (6 of 12 at 400; 2 of 10 at 500; 3 of 6 at 600; 1 of 3 at 700; and 2 of 2 at 800 mg/70 kg DXM).
Measures assessed at the end of the session, approximately 7 h after capsule administration
Pharmacological class questionnaire
Most volunteers (75%, 9 of 12) correctly identified placebo, although one participant each selected stimulant, classic hallucinogen, and other. Most volunteers also correctly identified triazolamas a sedative–hypnotic, with 66.7%(8 of 12) correct at the highest dose. DXM was dose-dependently identified as a classic hallucinogen (e.g., LSD, psilocybin, DMT,mescaline etc.); 91.7% (11 of 12) identified both the 400 mg/70 kg dose and their maximum dose as a classic hallucinogen.
Across all doses, DXM was relatively rarely identified as a dissociative anesthetic hallucinogen (e.g., like ketamine, DXM, PCP, etc.).
End of session rating of liking the experience
Triazolam did not increase end of session liking ratings, whereas DXM produced dose-related increases in liking, with significant effects at the penultimate and maximum DXM doses
Hallucinogen rating scale
DXM showed significant and generally dose-related increases on all six subscales of the HRS (Table 3). These effects included perceptual changes (e.g., visual and auditory hallucinations, illusions, and synesthesias), mood changes (e.g., feelings of transcendence, grief, joy, and/or anxiety), and cognitive changes (e.g., sense of meaning and/or ideas of reference). In contrast, the highest dose of triazolam (0.5 mg/70 kg) significantly affected only two of the six scales on the HRS (intensity of experience; impaired volition), both of which might be expected to be increased by a sedative-hypnotic drug.
Measures of mystical experience
Triazolam did not increase measures of mystical experience, whereas DXM produced dose-related increases on both the Mysticism Scale and the States of Consciousness Questionnaire. At the maximum dose of DXM, 7 of 11 volunteers (64%) met criteria on the States of Consciousness Questionnaire for having a “complete” mystical-type experience, and 2 of 11 (18%) met these criteria at the penultimate DXM dose. No volunteer met these criteria after placebo, the two doses of triazolam, or 100–300 mg/70 kg DXM.
Measures assessed 1 month after drug administration
Positive changes in attitudes about life and self, positive mood changes, positive social effects, positive behavior changes, and increased spirituality showed intermediate rates of endorsement which varied between 46 and 61% of maximum possible scores.
On the question probing how personally meaningful the session experiences were, 33% (4 of 12) of the volunteers rated the session experiences as “among the five most meaningful experiences of my life” and another 25% (3 of 12) rated the experiences as “among the 10 most meaningful experiences of my life”.
All 12 volunteers reported that study participation increased their current sense of personal well-being and life satisfaction.
One volunteer (8%) reported that his sense of personal well-being and life satisfaction increased “slightly” after study participation, seven volunteers (58%) reported it increased “moderately”, and four (33%) reported that it increased “very much”.
Of the 11 volunteers assessed for CYP2D6 status, one was a PM. No obvious differences with their data was seen. They received a max dose of 600 mg/70 kg.
COI: Lawrence Carter is an employee of Jazz Pharmaceuticals and owns stock and stock options in the company.
(Zawertailo, 2010) – Metabolic blockade of CYP2D6 decreases recreational properties of DXM
8 healthy subjects were exposed to DXM and quinidine/placebo in a single-blind placebo controlled manner.
Before each study day they received either placebo or quinidine 100 mg (oral) 10 hours before the DXM dose.
Depending on tolerability, the participants were exposed to higher doses on subsequent days, with washout days in between. The dose ranged from 1.3 mg/kg to 6 mg/kg.
All subjects were genotyped as homozygous (1/1) for the wild type allele, indicating extensive CYP2D6 metabolism.
Due to a lack of data, some doses could not be evaluated.
The drug conditions analyzed included:
Under placebo pre-treatment
Placebo (n=8)
2 mg/kg (n=7)
3 mg/kg (n=8)
4.5 mg/kg (n=6)
Under quinidine pre-treatment
DXM 2 mg/kg (n=7)
DXM 3 mg/kg (n=8)
DXM 4.5 mg/kg (n=4)
Results
Metabolism
Quinidine caused a 10-fold increase in the plasma concentration of DXM and a 10-fold decrease in the plasma concentration of DXO.
Drug effects
There was no effect of quinidine or DXM dose on AUC heart rate or blood pressure.
Pharmacological effects
Psychomotor performance
Significant dose-dependent decrement in performance scores for the manual tracking task and DSST with DXM.
Quinidine prior to 3 mg/kg DXM resulted in a significant decline in the performance on the manual tracking test, while pretreatment with quinidine did not alter the effect of other DXM doses.
Subjective effects-ARCI scales
ARCI subscales of mental sedation, physical unpleasantness, euphoria, and dysphoria increased dose-dependently with DXM.
Quinidine shifted the dose-response curve to the left for sedation and unpleasantness, along with causing a significant increase in AUC for physical unpleasantness, suggesting more pronounced negative effects with quinidine present.
Quinidine shifted the DXM dose-response downward for euphoria and significantly decreased total AUC, indicating less euphoria when CYP2D6 was inhibited.
Pharmacokinetic-Pharmacodynamic correlations
For the VAS “good effects” scale there was a positive correlation between unconjugated DXO concentration and VAS Clear Vision was negatively correlated with plasma DXM.
With DXM administered alone, there were some effects highly correlated with either plasma DXM or plasma unconjugated DXO.
For plasma unconjugated DXO: significant correlation with VAS “good effects” “bad effects” “floating” “awake” and “grounded”
For DXM concentrations: “strength of dose” and “duration of drug effect.”
COI: None
(Dickerson, 2008) – Reviewing Coricidin HBP (DXM and chlorpheniramine) abuse by adolescents
Retrospective review of hospital records from June 2001 – June 2004 from the inpatient child/adolescent psychiatric unit at Loma Linda University Medical Center in California.
Total of 47 adolescent patients with histories of Coricidin HBP abuse identified. Given an average of 1,450 patient admissions per year to that unit, that represents 1.1% of total admissions.
Mean age of 15.8.
Depression was the top psychiatric diagnosis (66%), then some also had psychotic disorders (13%)
Frequency of use ranged from experimentation to daily use. 37% reported at least once-weekly use.
Dose ranged from 2 to 42 tablets each time, with 63% taking a minimum of 8 tablets during each use.
85% took it to “get high” while 15% took it to attempt suicide.
Use was highly associated with alcohol and cannabis use.
Cardiac abnormalities
Two inpatients demonstrated significant cardiac abnormalities during their initial evaluation before ending up in the inpatient psychiatric unit. Neither had a history of prior medical problems.
These abnormalities may have been associated with the chlorpheniramine, along with DXM.
1
Took 8 Coricidin HBP tablets one day before evaluation. Presented with heart block on the ECG, BP of 155/85, and HR of 119.
2
Took 16 tablets two days before evaluation. Admitted to ICU with an ECG showing irregular heart rhythm with frequent premature ventricular contractions, bigeminy, and complaints of heart pounding.
COI: Not reported
(Ziaee, 2005) – Review of the effects of DXM abuse in Iranian young adults
58 volunteers with a mean age of 23.4. They had consumed DXM at least one time from March 2002 to December 2003 without medical indication.
18.9% had no history of medical DXM use while the others had used it for chronic cough and cold with physician’s prescription.
Frequency and duration
54.7% abused DXM more than 10 times and 52.8% had a history of abuse lasting over 3 years.
Mean frequency was 25.5 times and the mean first abused dose was 336.3 mg (75 – 1125 mg), while the mean last dose was 623.5 mg (90 – 2700 mg)
Acute effects
Autonomic
54.7% had sweating, 45.3% had tachycardia, 41.5% had fatigue, 28.3% had tachypnea, 28.3% had flushing, and 22.6% had a cool feeling
GI
30.2% had nausea, 24.5% vomiting, 7.5% diarrhea, 0% constipation
Pseudobulbar affect (aka pathological laughter and crying) occurs in a large portion of people with neurological disorders, such as amyotrophic lateral sclerosis (ALS), Alzheimer’s, and stroke (especially during the first year of recovery). It is believed to involve the disruption of circuits that are important for controlling appropriate emotional responses. There may be a lack of cortical inhibition, thereby triggering inappropriate functionality from the cerebellum and/or brain stem.
Some evidence points to abnormalities involving serotonin, dopamine, glutamate, and sigma (σ) receptors. σ receptors, for which DXM is a ligand and agonist, are concentrated in the cerebellum and brain stem, which could contribute to its efficacy.
None of the historically popular drugs for PBA (SSRIs, TCAs, and dopaminergic agents) have been approved by the FDA for that condition, but a combo of DXM and quinidine (Nuedexta) was approved in 2010. That combination includes 20 mg DXM with 10 mg quinidine and is typically used twice per day.
Three controlled trials demonstrated efficacy, with one showing a 51% remission rate at 12 weeks compared to 29% with placebo (Schoedel, 2014). Early reports used up to 75 mg quinidine and indeed higher amounts than 10 mg are needed for full CYP2D6 inhibition, but it does not appear higher quinidine doses are needed to enhance DXM’s efficacy. Schoedel (2014) reports just adding 10 mg to DXM 30 mg can produce a 20-fold or greater increase in DXM plasma concentrations vs. DXM alone (64-114 ng/mL vs. around 2 ng/mL). While the mean peak quinidine concentration is just a fraction of the amount used for arrhythmias, so it should have a low chance of affecting heart function. Clinical studies support the cardiovascular safety of the combination, showing it can slightly prolong the QTc interval but otherwise doesn’t have a clinically significant effect.
Most of the PBA studies have focused on Alzheimer’s, ALS, and multiple sclerosis (MS), but it was also effective in dementia patients (Doody, 2016), where it produced a 31.4% remission rate at Day 90 and a reduction in PBA episodes from 21 per week to 3 per week.
Because the combination of DXM and quinidine is significantly more effective than DXM alone (Smith, 2006), it seems likely DXM itself is the important substance, not dextrorphan (DXO) or another metabolite.
Evidence from the ALS population also indicates the drug can simultaneously improve anger and frustration symptoms (Smith, 2006).
It is typically well-tolerated. A safety trial of 553 patients with PBA from various conditions showed 30 mg DXM with 30 mg quinidine twice daily produced no clinically significant heart rate (HR), blood pressure (BP), respiration, or temperature changes (Pattee, 2014). The most common adverse effects were nausea, headache, dizziness, falls, and diarrhea.
(Doody, 2016) – Open-label trial showing efficacy in PBA in dementia patients
Open-label 90-day trial. DXM and quinidine were given at 20 mg and 10 mg twice daily.
Patients had a clinical diagnosis of dementia (including Alzheimer’s disease, or vascular, Lew Body, or frontotemporal dementia) and a clinical diagnosis of PBA.
The primary efficacy measure was change in CNS-LS score from baseline to Day 90.
Results
134 patients were enrolled, received at least one dose, and were included in the safety population. Of those, 79.1% completed the study and 20.9% did not.
10.4% didn’t complete due to adverse events and 5.2% did not complete due to withdrawal of consent.
A total of 26 (19.4%) of enrolled patients were excluded from efficacy analyses, 16 because they lacked a post-baseline efficacy reading and 10 because they did not meet all study eligibility requirements.
This means 108 (80.6%) were in the effectiveness population.
Demographics
Mean age: 70.7
Diagnosis: 64.2% had probable Alzheimer’s, 15.7% had vascular dementia, 9.0% had frontotemporal dementia, and 3.7% had Lewy body dementia, with the other 7.46% having “other” dementia diagnosis.
93.3% were assessed as having mild to moderate severity dementia.
They were taking a median of 8 medications, with 81.3% taking at least 1 psychopharmacologic medication, most often antidepressants (56.7%), benzodiazepines (34.3%), or antipsychotics (29.1%).
Efficacy
There was progressive, significant improvement on the CNS-LS. The reducations at Day 30 (-4.6) and Day 90 (-7.2) were significant. The Day 90 reduction fell within the 95% CI for CNS-LS reduction seen with the same medication in a pivotal Phase 3 trial that was placebo-controlled in patients with PBA secondary to ALS or MS. And the reduction was below the lower limit of the 95% CI for the CNS-LS reduction seen with placebo in that trial.
The median PBA episodes/week declined from 21 at baseline to 6 at Day 30 and 3 at Day 90.
Overall, the estimated number of PBA episodes in the week before assessment was down 50.2% at Day 30 and 67.6% at Day 90.
Remission (no reported episodes in the week before assessment) occurred in 31.4% by Day 90.
On the Patient Treatment Satisfaction Survey, 74.5% of patients or their caregivers were somewhat satisfied (21.6%) or very satisfied (52.9%), while 11.8% were somewhat dissatisfied or very dissatisfied. The remaining 13.7% had a neutral response.
Safety
36.6% of the 134 patients had at least 1 treatment-emergent adverse event. The most common ones were headache in 7.5%, urinary tract infection in 4.5%, and diarrhea in 3.7%.
10.4% of patients had a serious adverse effect, including 2 patients who died. But neither fatality was considered related to the medication.
COI: The study was funded by Avanir Pharmaceuticals. Authors have consulted for pharmaceutical companies, worked for pharmaceutical companies, have stock options, and have woorked on trials funded by pharmaceutical companies. Authors have worked in some way with Avanir.
(Pattee, 2014) – DXM/Quinidine is well-tolerated in PBA
Open-label multicenter study over a 52-week period.
DDXM/Quinidine given orally at 30 and 30 mg once daily in the evening for the first week and then twice daily after that.
553 patients with PBA from over 30 neurological conditions, often ALS or MS.
Results
The most frequent adverse effects (over 15%) were nausea, headache, dizziness, fall, and diarrhea.
Most adverse effects deemed related to treatment were mild-to-moderate in severity.
Lab tests remained stable during the trial and there were no clinically significant alterations of BP, HR, respiration, or body temperature.
Pharmacokinetics
Mean plasma concentrations:
DXM: 92.7 ng/mL
DXO: 78.0 ng/mL
Quinidine: 0.15 μg/mL
COI: Funding provided by Avanir Pharmaceuticals. And some authors served on speakers bureaus and received financial support from Avanir Pharmaceuticals.
(Schoedel, 2014) – Review of DXM with quinidine
Efficacy of DXM/Quinidine for PBA
3 controlled trials of DXM/Quinidine have indicated efficacy.
One (the US registration trial that resulted in approval) showed a 49% drop in PBA episode rate compared to placebo overall. More DXM/Quinidine patients were in remission at 12 weeks vs. placebo (51% vs 29%).
All trials showed highly significant declines in core symptoms and other clinically relevant outcomes like decreased episode count, quality of life, functioning, and interactions with others.
One of the trials showed a significant improvement on the BDI-II for depression, though without a significant improvement on the Neuropsychiatric Inventory.
Evidence indicates the 30/10 mg vs. 20/10 mg group have have responded a little earlier.
Safety considerations with DXM/Quinidine
General safety in clinical trials
The most common adverse effects with a greater frequency vs. placebo: dizziness, fatigue, nausea, and weakness.
One of the studies showed nausea in 11.8%, dizziness in 10.5%, headache in 9.9%, somnolence in 7.2%, fatigue in 7.1%, diarrhea in 6.5%, and dry mouth in 5.1%.
Some data even suggested adverse effects can sometimes be lower in the active group, such as dermatitis, fatigue, aggravation, headache, and pain in limbs.
Multiple sclerosis patients often report disabling pain. Since decreased glutamatergic could alleviate pain, the lower reports of pain in limbs are particularly interesting.
Discontinuation rates due to adverse effects in the multiple sclerosis study was lower than in the ALS study (24%). In the ALS study, discontinuations mainly came from musculoskeletal complaints that were not present in the multiple sclerosis patients.
COI: Authors provided consultation to Avanir Pharmaceuticals. Authors have been independent consultants to Avanir Pharmaceuticals. No other conflicts reported.
(Panitch, 2006) – DXM/Quinidine is effective in the treatment of pseudobulbar affect in multiple sclerosis
DXM given twice daily for 12-weeks. Double-blind, placebo-controlled study.
30 mg/30 mg of DXM and quinidine per dose
150 patients with multiple sclerosis.
Results
Patients receiving the drug had greater reductions in Center for Neurologic Study-Lability Scale scores vs. placebo at all clinic visits during the 12 weeks. All secondary end points also favored DXM/quinidine, including number of crying or laughing episodes, quality of life, quality of relationships, and pain intensity score.
Tolerability
It was well-tolerated. Only dizziness occurred significantly more frequently and it was usually mild, with only one case of severe dizziness.
No significant difference in the number of patients who discontinued the study or stopped medication.
No significant difference between groups for ECG parameters.
DXM/quinidine resulted in sustained, therapeutic levels of DXM in plasma during the 12-week period and higher DXM levels correlated with decreased symptoms.
COI: Funded by Avanir Pharmaceuticals
Emotional Lability
Case reports have indicated it may be useful in emotional lability, such as depression (Messias, 2012).
(Messias, 2012) – Case report of benefit in emotional lability associated with depression
32-year-old female with a history of depression. Long history of psychiatric problems, including suicide attempts.
Failed to respond to multiple classes of antidepressants over a long period of time. Psychotherapy was not entirely effective, nor was ECT.
Despite trying 11 sessions of ECT, she was still reporting problems in controlling her affective expression, especially crying outbursts.
She began treatment with DXM and quinidine (20 mg and 10 mg) daily. At the start, she had a score of 14 on the Center for Neurologic Study Lability Scale (over 10 is indicative of lability)
After a year of treatment, she reported significant improvements in mood lability and crying spells. At the time of writing, she had been out of the hospital and was able to go to work daily. She felt her affective control allowed her to benefit from psychotherapy.
COI: Not reported
Neuropathic Pain
NMDA antagonists like DXM are of interest in general for pain, but the outcomes have varied substantially between studies, doses, and specific conditions. Even if DXM is effective, the dose required may prove intolerable for many patients due to effects like sedation, dissociation, and dysphoria. There is limited evidence that DXM is highly useful in neuropathic pain.
Carlsson (2014) studied 13 patients with neuropathic pain in a DBRCT. They received 270 mg DXM or placebo. There was a significant beneficial response compared to placebo (average of 30% decline in pain), but with marked variation between patients.
A 6-week trial with an average of 381 mg/d found it could reduce pain in diabetic neuropathy (average of -24% in 13 patients), but not postherpetic neuralgia (average of -2% in 13 patients) (Nelson, 1997). The authors hypothesized DXM might be more effective when there is ongoing damage to nerves (i.e. diabetic neuropathy) compared to conditions with a fixed lesion (i.e. postherpetic neuralgia).
It failed to improve facial neuralgias like possible trigeminal neuralgia, anesthesia dolorosa, and idiopathic trigeminal neuralgia in a DBRCT with a mean dose of 178-640 mg/d depending on the condition (Gilron, 2000).
Cohen (2004) demonstrated some efficacy in 25 patients with pain usually stemming from failed back surgery syndrome, complex regional pain syndrome, or peripheral neuropathy. The study also found the acute response to ketamine 0.1 mg/kg IV was predictive of a patient’s later response to chronic DXM (titrated up to 1 mg/kg per day). Based on a response criteria of 67% pain reduction for ketamine and 50% pain reduction for DXM, 9/25 responded to both drugs, 12 failed with both, and 3 responded to DXM but not ketamine. The positive predictive value was 90% and the negative predictive value was 80%. Importantly, placebo response correlated with medication response. Placebo responders were significantly more likely to respond to ketamine (70% vs 20%) and DXM (70% vs. 33%).
A study of 19 patients with chronic pain from stroke or post-surgical neuralgia showed no benefit from 13.5 mg three times per day or 27 mg three times per day (McQuay, 1994).
(Carlsson, 2004) – Some benefit in neuropathic pain
15 patients with post-traumatic neuropathic pain (avg duration of pain = 6 years). Assigned in a placebo-controlled, double-blind, randomized crossover manner.
They received either 270 mg DXM hydrobromide or placebo.
1 patient discontinued on the first day (DXM) due to unacceptable side effects. Another was excluded due to a baseline VAS value for pain that was too low. So the results are based on the remaining 13 people.
Since just 4 were PMs and 9 were EMs, it’s difficult to truly evaluate the contribution of metabolism.
Results
Significant analgesic effect vs. placebo, but with marked variation between patients.
Extensive metabolizers had an apparently superior analgesic effect than poor metabolizers, who received comparatively lower relief, sometimes with no effect (but little/no effect was also seen in some EMs).
On average, there was a 30% decline in pain vs. placebo. The difference vs. placebo was significant after 1.5 hours and more significant after 2.5-4 hours. The first reduction in pain occurred around 1 hour, lasting for 2-3 hours after that point.
Adverse
Most had adverse effects like light-headedness and drowsiness (though drowsiness was also common in placebo). Visual disturbances and hot flushes were also common.
Light-headedness was the most important adverse effect noted.
Unlike analgesia, the intensity of adverse effects did not seem to differ between PMs and EMs.
For some, both the analgesia and adverse effects persisted the entire day. And a few patients experienced adverse effects for several days post-DXM.
COI: Not reported
(Cohen, 2004) – DXM is effective in some patients and acute ketamine injection response is predictive of later oral DXM response.
Small dose 0.1 mg/kg IV ketamine was studied and then compared to oral DXM treatment regimen. DXM dose started at 0.5 mg/kg oral twice daily, titrating up to 1 mg/kg twice daily over a two-week period as tolerated.
25 patients were studied.
7 had failed back surgery syndrome with a radicular component, 5 had complex regional pain syndrome type 1, 4 had peripheral neuropathy, 2 had central pain, and 2 had postherpetic neuralgia.
Results
9 responded to both, 12 failed with both, 1 responded to ketamine but not DXM, and 3 responded to DXM but not ketamine.
With a response cutoff of at least 50% pain reduction from ketamine: 64% positive predictive value, 73% negative predictive value, and observed agreement of 68%.
With a response cutoff of at least 67% pain reduction from ketamine: 90% positive predictive value, 80% negative predictive value, and 84% observed agreement.
Placebo responders were significantly more likely to response to both ketamine (70% vs 20%) and DXM (70% vs. 33%) than nonplacebo responders.
3/12 DXM responders failed to respond to ketamine.
Negatives
19 were confused or euphoric after ketamine, with 1 complaining of nausea.
5 with DXM reported nausea and/or vomiting; 1 developed a rash after 16 days forcing her to stop treatment; 1 patient had urinary retention at 240 mg/d that required dose reduction to 180 mg/d; 1 had poor pain relief and hallucinations at 210 mg/d.
Of the 19 reporting side effects with ketamine, 7 reported side effects with DXM.
COI: Not reported
(Gilron, 2000) – Failed to improve facial neuralgias
The patients in the study had idiopathic trigeminal neuralgia, anesthesia dolorosa, or symptoms suggestive of possible trigeminal neuralgia.
All needed to have gone through a prior trial of carbamazepine or baclofen (for trigeminal neuralgia) or a TCA, opioid, or gabapentin (for other neuralgias)
Treatments
DXM was compared to the active placebo lorazepam in a randomized, double-blind, crossover manner. Patients were studied during 6-week treatment periods.
Drugs
DXM at 120 mg/d in four divided doses titrated to a max of 920 mg/d.
Lorazepam was given at 0.24 mg/d in four divided doses then titrated to a max of 1.84 mg/d.
A total of 19 patients (11 with possible trigeminal neuralgia, 5 with anesthesia dolorosa, and 3 with trigeminal neuralgia) were enrolled. 16/19 completed both treatments.
One of the patients dropped out after 26 days in the first treatment period (with DXM) due to intolerable sedation.
Results
Facial pain with possible trigeminal neuralgia
Mean dose: 357 mg/d for DXM and 1.2 mg/d for placebo. In the last two weeks of the treatment period, there was only slightly less pain with DXM, which was not significant. A 4% decline in pain was the mean.
Anesthesia dolorosa
The mean does was 178 mg/d for DXM and 1 mg/d for placebo. In the last two weeks, there was no significant benefit with DXM, it was only correlated with slightly less pain.
Idiopathic trigeminal neuralgia
Mean dose: 580 mg/d and 640 mg/d for the two patients on DXM, respectively (compared to 1.16 mg/d and 1.84 mg/d for placebo)
There was less pain with a decline of 37%, but this was still not significant (p=0.36)
COI: Funding was a grant from the National Institute of Dental and Craniofacial Research.
(Nelson, 1997) – Somewhat useful in diabetic neuropathy, but not in postherpetic neuralgia
6 weeks of therapy. Patients with either painful diabetic neuropathy or postherpetic neuralgia
Drugs compared in a RCT, two-perid, crossover manner
Beginning at 120 mg in four divided doses. Titrated top a max of 960 mg/d.
Due to concerns about Olney’s lesions, patients were also given 0.5 mg benztropine daily.
Results
Diabetic neuropathy
13 patients completed both treatments. Median disease duration of 13 years and pain duration was 4 years.
In the last week of treatment, the average dose was 381 mg/d
In the last week of the trial, DXM reduced pain (based on the 13-word descriptor scale) by a mean of 24%.
Global pain relief ratings:
DXM group: “a lot” in 4, moderate in 3, slight in 4, none in 2, and pain worse in 0.
Placebo: A lot in 0, moderate in 0, slight in 6, none in 5, and pain worse in 2.
No patient had full pain relief with either treatment.
6/7 reporting moderate or better global pain relief with DXM reported their lowest weekly mean pain score at the highest DXM dose tolerated.
Postherpetic neuralgia
13 completed both treatments, but 18 were randomized, with 5 dropping out due to sedation (3), ataxia (1), confusion (1), and sixth cranial nerve palsy unrelated to drug treatment (1).
Median pain duration was 2 years
Average dose at the end: 439 mg/d
In the last week of treatment, placebo patients had slightly less pain (based on the 13-word descriptor scale). Difference was a mean of 2%
Global pain relief ratings:
DXM: A lot in 1, moderate in 4, slight in 5, none in 2, and pain worse in 1
Placebo: A lot in 2, moderate in 1, slight in 3, none in 5, pain worse in 2.
4 patients taking regularly prescribed opioids during the study weren’t among those with a positive DXM response. All favored placebo.
Adverse effects
Every patient given DXM had side effects, while only 1 patient reported side effects during placebo.
18/31 given DXM reported sedation during the titration phase. This caused 3 to withdraw and 7 to reduce their dose.
By the maintenance phase, only 9 continued to report sedation
COI: Not reported
(McQuay, 1994) – Ineffective in neuropathic pain
19 patients with chronic neuropathic pain. They continued their existing medications, including opioids and antidepressants. Most had neuropathic pain in the form of post-stroke pain or postsurgical neuralgia.
Studied the effects in a multiple-dose, double-blind randomized controlled cross-over comparison of 13.5 mg t.d.s vs. placebo t.d.s in a 10-day treatment period. And in a second 10-day period there was a 27 mg DXM t.d.s vs. placebo.
The study incorporated a 5 pair n-of-1 design for each dose.
Results
No significant differences between DXM and placebo on any outcome measure. 2 patients had significantly better analgesia on one outcome, one with DXM and one with placebo.
10 had no adverse effects with either DXM dose. 2 withdrew during the first period because of adverse effects, including increased pain. And 5 withdrew during the second period.
5 patients continued with DXM after the study for 1-3 months, largely not receiving benefit.
COI: Not reported
Animals
(Morel, 2014) – DXM appears useful in a model of neuropathic pain
Rats. Drugs administered via IP. DXM 10 mg/kg or memantine 20 mg/kg.
Results
DXM, but not memantine, reversed tactile allodynia
It significant increased the nociceptive thresholds of 50% response. Neither placebo nor memantine did.
DXM, but not memantine, reversed mechanical hyperalgesia
It significantly increased vocalization thresholds.
DXM, but not memantine, restores spatial memory integriry
Rats treated with DXM showed a significant increase in the % of time spent in the novel arm vs. animals given saline.
DXM, but not memantine, is associated with less NR2B-NMDAR subunit phosphorylation
NR2B is a subunit of the NMDA receptor.
There was a significant decline of pTyr1336NR2B in the spinal cord of DXM-treated animals, but DXM did not significantly alter phosphorylation of Tyr1472NR2B.
(Wang, 2009) – DXM combined with melatonin can reduce neuropathic pain in rats
Rats with chronic constriction sciatic nerve injury (CCI).
The Wistar-Kyoto rats used in the study are hypersensitive to stress, have been used to study depression, and exhibit overall decreased activity, few exploratory behaviors, hypolocomotion, and a high level of behavioral immobility in the forced swim test.
Previous research showed these rats have an exacerbation of mechanical allodynia after CCI that could be prevented by melatonin administration into the contralateral anterior cingulate cortex.
DXM and/or melatonin were given to rats once daily for a week via IP injection.
DXM alone (15, 30, and 60 mg/kg) was able to reduce thermal hyperalgesia and it reduced mechanical allodynia at 30 and 60 mg/kg.
Whereas melatonin alone was only effective for reducing thermal hyperalgesia at the highest tested dose of 120 mg/kg, not at 30 or 60 mg/kg.
Melatonin was ineffective at all doses for reducing mechanical allodynia.
The combination of melatonin 30 mg/kg with DXM 15 mg/kg led to an effective reversal of both thermal hyperalgesia and mechanical allodynia, while neither drug at those doses was effective individually.
COI: Not reported.
Study supported by NIH grants DE18214, DE18538, and NS45681
General Analgesia
NMDA antagonists may offer some pain relief on their own, though they may have a higher efficacy when used to enhance opioids. DXM could reduce opioid tolerance and/or boost the effects of each opioid dose, allowing people to use less.
The rodent evidence of benefit is plentiful. DXM potentiates mu opioid receptor (MOR) agonists and delta opioid receptor (DOR) agonists, while not improving the effects of kappa opioid receptor agonists (KOR) (Chen, 2005; Baker, 2002; Plesan, 1998; Hoffmann, 1996). It’s been found to have an effect at 10 – 45 mg/kg in rodents, usually given SC or IP.
It potentiated MOR and DOR agonists in monkeys at 1-10 mg/kg IM, while not increasing the incidence of sedation or motor problems (Allen, 2002).
Though it was able to potentiate morphine and meperidine, Chen (2005) found it did not potentiate codeine, perhaps due to DXM being a CYP2D6 substrate and codeine relying on 2D6-dependent metabolism to morphine for much of its benefit.
Some studies indicate it can be given after repeated morphine administration to reduce tolerance. Mao (1996) showed tolerance developed to morphine 32 mg/kg oral within five days, but pairing it with a 2:1, 1:1, or 1:2 ratio of DXM could return morphine’s activity to a baseline level. Not all studies support its tolerance-reducing effects (Hoffmann, 1996).
Morphine also enhanced the effects of NSAIDs like ibuprofen and naproxen in rats at 50 mg/kg oral, again without offering antinociception on its own.
Another source of antinociception in rodents is swim-stress. DXM at as little as 1.25 mg/kg in mice could enhance swim-stress-induced antinociception, yet it did not alter the development of tolerance to that form of antinociception (Fazli-Tabaei, 2008).
Human Research
When we look at human research, the literature is less clear. DXM typically isn’t a good analgesic on its own and it may not even potentiate opioids, at least at the doses used so far.
It failed to improve the effects of slow-release morphine when given at 60-120 mg four times per day (Dudgeon, 2007) and three large 3-month clinical trials in non-malignant pain showed no benefit of adding DXM to morphine for efficacy or tolerance (Galer, 2005). The Galer study used 45 to 360 mg per day.
Mercadante (1998) found no benefit in neuropathic or nociceptive pain syndromes associated with cancer when given at 30 mg three times daily.
A detailed study from Cohen (2006) found it offered pain relief on its own in fibromyalgia at up to 1 mg/kg three times daily, but only for a minority of patients. It also showed that people’s acute response to a ketamine injection was predictive of their later response to daily DXM. Of 34 patients, 10 were responsive to both drugs (defined as >50% pain relief with DXM and >67% pain relief with ketamine), 19 responded to neither, 2 responded to DXM but not ketamine, and 3 responded to ketamine but not DXM. Importantly, the average pain score was significantly lower in people who also responded to placebo vs. nonresponders.
Human
(Dudgeon, 2007) – Lack of benefit in cancer pain when used with morphine
65 patients. DXM at 60-120 mg four times daily with slow-release morphine.
Only non-significant differences in morphine use and pain scores.
COI: Not reported
(Cohen, 2006) – Sometimes effective in fibromyalgia and acute ketamine injection is predictive of later DXM response.
0.5 mg/kg DXM three times daily, up to 1 mg/kg three times daily.
34 patients: 10 responsive to both, 19 responsive to neither, 2 responsive to DXM but not ketamine, 3 responsive to ketamine but not DXM.
Average response was significantly higher in placebo responders vs placebo non-responders.
COI: Not reported
(Galer, 2005) – Three large trials for 3-months each in chronic, non-malignant pain failed to show any benefit of adding DXM to morphine in chronic pain. Neither efficacy nor tolerance was improved.
Doses ranged from 45 to 360 mg/d.
COI: Paper completed by employees of Endo Pharmaceuticals
(Mercadante, 1998) – DXM is not effective in cancer pain
58 patients. 30 mg three times daily. Equally ineffective in neuropathic and nociceptive pain syndromes.
COI: Not reported
Animal
(Fazli-Tabaei, 2008) – DXM alters the impact of the swim-stress on antinociception and antinociception tolerance in mice
5 mg/kg. Lack of benefit from 2.5 mg/kg on its own, though it improved swim-stress antinociception with as little as 1.25 mg/kg.
DXM produced antinociception on its own and also increased the benefits of swim-stress on nociception, but it failed to alter the development of tolerance to antinociception from swim-stress.
COI: Not reported
(Chen, 2005) – Showing an impact on opioid antinociception in rats.
Co-administering DXM 20 mg/kg IP with some MOR agonists (morphine, meperidine) produced an increase in effects. It didn’t boost the effect of codeine or KOR agonists. It also raised the serum concentration of morphine.
May not boost codeine due to it being a 2D6 substrate and inhibiting morphine formation from codeine.
COI: This study was supported by the grant from National Health Research Institutes, Taiwan, R.O.C. (NHRI-EX-92-8909BP) and was supported in part by the C.Y. Chai Foundation for Advancement of Education, Science and Medicine, Taiwan, R.O.C.
(Baker, 2002) – DXM potentiates antinociception from MOR agonists, but not KOR or DOR agonists
DXM given at 10 and 20 mg/kg
COI: Not reported
(Allen, 2002) – Potentiates analgesia from MOR and DOR agonists.
4 squirrel monkeys. DXM via IM. Alone it failed to induce antinociception. But 1.0-10 mg/kg was able to make otherwise ineffective morphine doses effective. It also potentiated a DOR agonist.
COI: This work was supported by U.S. Public Health Service R37-DA02749 (to L.A.D.) and Research Scientist Award DA00033 from the National Institute on Drug Abuse
(Plesan, 1998) – DXM enhances antinociception from morphine in rats
DXM 1 and 5 mg/kg SC didn’t potentiate morphine but 15, 30, and 45 mg/kg did dose-dependently improve the effects of morphine both in magnitude and duration. It did not increase sedation or motor deficits from morphine.
COI: Supported by the Swedish Medical Research Council, the Swedish Institute, Astra Pain Control AB, and the Biomed 2 program of the European Commission.
(Hoffmann, 1996) – DXM potentiates morphine antinociception but not doesn’t reverse tolerance in rats
DXM 30 mg/kg
DXM and morphine alone didn’t have an effect in opioid-tolerant rats. But antinociception from the combo was significantly higher than with morphine alone.
COI: Not reported
(Price, 1996) – Enhances the analgesic effect of NSAIDs in rats, but doesn’t offer its own analgesia.
Oral DXM 12.5-100 mg/kg failed to significantly offer pain reduction, but adding 50 mg/kg to ibuprofen led to significantly greater analgesia (around 2x greater pain relief).
Similar when adding it to other NSAIDs, including naproxen.
COI: Supported by Algos Pharmaceutical Corporation.
(Mao, 1996) – DXM enhances antinociception from morphine and attenuates its tolerance
Rats. Morphine given at 32 mg/kg oral, which led to tolerance after 5 days. Then tested in 2:1, 1:1, and 1:2 combos with DXM. Combo group showed significantly greater effect from morphine post-Day 5, with responses not differing significantly from Day 1.
Even in the highest morphine to DXM group (4:1), response on Day 8 was significantly higher than morphine-only.
DXM itself at 64 mg/kg was able to offer some antinociception but it was significantly less than with morphine.
When given on Day 1 with morphine, it increased antinociception at lower doses in a MS/DXM ratio of 1:2 or 2:1 with 15 mg/kg morphine. Higher 24 or 32 mg/kg morphine doses were not enhanced by morphine.
COI: Supported by an award from Algos Pharmaceutical Corporation.
Surgical Pain
DXM shows promise in surgical pain, with a number of studies indicating perioperative administration can reduce pain after or during an operation, which facilitates a reduction in opioid need. Some negative studies do exist, but overall DXM tends to show an effect, mostly when given prior to an operation.
This benefit may come from reducing spinal cord arousal. A sufficiently large acute stimulus (like surgery) could lead to sensitization of dorsal horn neurons and therefore a lower threshold for sensing pain. NMDAR channel opening could play a role in this sensitization, which is where the NMDAR blocking effect of DXM comes into play, though other aspects of its pharmacology could also play a role.
Studies investigating its mechanism have shown acute pain relief is not provided at 0.5 mg/kg IV, but it is able to reduce hyperalgesia (Duedahl, 2005).
A review of its perioperative use found it did reduce the need for conventional analgesics when given at 90 mg oral or 40 mg IM, though the reduction in opioid use (i.e. 10-20 fewer milligrams of morphine) is of unclear clinical utility (King, 2016). It also reduced pain scores 1-24 hours after surgery.
Some studies have shown especially large effects, such as reducing morphine use by an average of 50% and allowing a fair portion of patients to go without postoperative opioids (Weinbroum, 2001). While others have failed to show any postoperative benefit (Grace, 1998). Differences in the type of operation and dose could account for some of the variations in efficacy.
(King, 2016) – Review of DXM perioperatively. It does improve reduce the need for conventional analgesics. Though the changes, such as 10-20 mg less morphine is of unclear clinical utility.
Doses tended to be around 90 mg oral or 40 mg IM preoperatively. Total of 21 studies evaluated.
DXM produced a reduction in IV morphine need after surgery (p=0.0006) and if a couple outlier studies with larger effects are removed, it’s still significant (p=0.004).
DXM was favored for pain scores 1-24 hours after surgery.
A dose-related effect was found.
COI: None
(Duedahl, 2006) – It seems to improve outcomes when given perioperatively, but the results are variable between studies and of unclear clinical relevance.
28 DBRCTs. 1629 patients (906 receiving DXM).
There were at least significant pain score differences at 1 and 2 hours, with smaller though significant differences in the 4-6 hour postoperative period.
Appears to prolong the time until a patient needs opioids by several hours. Clinical relevance overall is unclear given the magnitude of opioid use reduction and pain score reduction is not massive.
COI: Not reported.
(Hasan, 2004) – Reduction in opioid use in children postoperatively
38 children. Placebo-controlled. Operation: tympanomastoid surgery. Given DXM (1 mg/kg up to max of 60 mg) or placebo one hour prior to surgery.
Significantly lower fentanyl use during surgery (2.6 μg/kg vs. 4.1 μg/kg) and morphine use during hospital stay (73 μg/kg vs. 150 μg/kg). Max pain score was also lower. No significant difference in vomiting and nausea rate.
COI: Not reported
(Weinbroum, 2002) – DXM offers pain relief when given before surgery
Patients received placebo, DXM 60 mg, or DXM 90 mg before surgery and two days after. Surgery for bone and soft tissue malignancies.
Patients receiving DXM (either dose) had similarly lower pain scores (50-80%). This was seen both immediately and up to 3 days postoperatively.
There was a 50% decline in estimated overall maximum pain intensity.
Both groups used 50-70% less morphine than placebo patients.
DXM patients were also an average of 70% less sedated.
COI: Not reported
(Weinbroum, 2001) – Pre-incisional DXM with epidural lidocaine improves postoperative pain and opioid need
DBRCT. Inguinal herniorrhaphy or surgical anthroscopy under epidural lidocaine. Either 90 mg, 60 mg, or placebo.
53 patients. Mean morphine use was ~50% that of the placebo group. 10/33 DXM patients received no morphine, compared to 0/20 placebo patients.
Pain was reported to be higher in placebo patients vs. 60 mg patients, though no significant difference for placebo vs. 90 mg.
60 mg was found to be the best dose, with 90 mg less effective in some regards.
COI: Not reported
(Weinbroum, 2000) – DXM is effective if given preoperatively. It can reduce postoperative pain and secondary thermal hyperalgesia.
30 patients. Laparoscopic cholecystectomy or inguinal hernioplasty. DXM 90 mg oral or placebo 90 min pre-anesthesia.
Mean morphine use by weight was significantly lower and diclofenac injection rate was around 55% lower vs. placebo (diclofenac was given rather than morphine after Hour 6).
DXM patients were also less affected by cold/heat sensations near their incision, while placebo patients showed a reduced threshold for registering the sensation. DXM therefore may protect against thermal hyperalgesia and hyperpathia.
COI: Not reported
(Henderson, 1999) – Perioperative DXM can reduce postoperative pain after hysterectomy
Double-blind study of 47 females. Given DXM 40 mg 90 min before surgery, 40 mg the evening after, and 40 mg three times daily for the next 2 days.
Median general pain score was lower, but no significant difference on pain during movement. Non-significant reduction in morphine use during the first 24 hours, but significantly lower opioid/paracetamol use during the next two days, without a significant difference in diclofenac usage (diclofenac was the main opioid during those days).
COI: Not reported
(Wu, 1999) – Preincisional DXM is more effective than post-surgical DXM for reducing pain and opioid use after laparoscopic cholecystectomy
DXM 40 mg w/ chlorpheniramine 20 mg IM either 30 min before or postoperative.
Preoperative DXM showed significantly delayed time to opioid need (28.6 hours vs. 9.3 hours), significantly lower opioid use (20.0 mg meperidine vs. 90.7 mg), and lower pain score (4.0 vs. 6.0).
COI: Not reported
(Grace, 1998) – DXM preoperatively does not improve post-surgical outcomes, but it does reduce intraoperative morphine use.
37 patients undergoing surgery requiring laparotomy. 60 mg DXM or placebo the night before and 1 hr before surgery.
DXM group used less morphine intraoperatively, 13.1 vs. 17.6 mg. But no significant difference at any point postoperatively. No significant pain score difference postoperatively.
COI: Not reported
Diabetes
Because there are glutamatergic receptors in the pancreas, NMDAR antagonists could play a role in diabetes treatment. A couple studies have found it improves pancreatic function by raising glucose stimulated insulin secretion (GSIS), perhaps without affecting basal insulin levels, which helps to decrease the chance of a hypoglycemic event. Hypoglycemia has historically been a problem with diabetes treatments like the sulfonylureas.
Marquard (2015) found support for the antidiabetic properties of DXM and DXO in an in vitro and animal model study. Those NMDAR antagonists were shown to increase GSIS without affecting basal insulin secretion. Metabolites like 3-hydroxymorphinan and 3-methoxymorphinan were also beneficial. DXM’s efficacy is associated with the NMDA receptor since mice lacking that target showed no beneficial impact.
Chronic treatment in mice (specifically those operating as a model of type 2 diabetes) with DXM added to drinking water (3 mg/mL) for three weeks resulted in significantly lower fasting blood glucose concentrations compared to 1 mg/mL (Marquard, 2015). At 12 weeks of age, mice given 3 mg/mL had significantly improved glucose tolerance and fasting blood glucose. Islet insulin content increased and the areas of insulin-expressing beta cells and glucagon-expressing alpha cells were more than twice as large with 3 mg/mL vs. 1 mg/mL.
A second study from Marquard demonstrated beneficial effects in humans. 20 participants with type 2 diabetes were given 30, 60, or 90 mg DXM with or without 100 mg sitagliptin (Marquard, 2015). A placebo control was also used. The effects of DXM and sitagliptin were studied by conducting an oral glucose tolerance test an hour after drug administration. DXM alone caused a small reduction in glucose (less of an effect than sitagliptin alone), while DXM+sitagliptin showed lower values of glucose compared to sitagliptin alone.
All DXM doses non-significantly increased max insulin levels postprandially, whereas sitagliptin alone and sitagliptin+DXM significantly raised insulin levels (Marquard, 2015). 90 mg DXM with sitagliptin was significantly more effective than sitagliptin alone. Sitagliptin alone produced a 30-min AUC increase of 50%, while it was 110% once 30 or 60 mg DXM was added. Although the combo significantly increased insulin levels during the first 30 min of the test, they were not increased at all during the last two hours of the test.
(Marquard, 2015) – DXM can lower blood glucose and raise insulin levels in people with Type 2 diabetes.
20 males with T2DM who were stable on a regimen of metformin monotherapy for at least 3 months.
Drugs: Either 30/60/90 mg DXM, 100 mg sitagliptin, 30/60/90 mg DXM + 100 mg sitagliptin, or placebo.
One hour after study drug administration the participants were put through an oral glucose tolerance test with 75 g glucose.
Results
DXM produced a small nonsignificant reduction in max blood glucose concentration and AUC1-3h blood glucose.
Whereas DXM + sitagliptin showed numerically lower values of blood glucose vs. sitagliptin alone, both for AUC1-3h and AUC3-5h
For all DXM doses added to sitagliptin, blood glucose reductions within 4 h after starting the test of 8.9, 10.5, and 10.7% were seen, compared to 6.5% with sitagliptin alone.
Postprandial serum insulin
All DXM doses vs. placebo were found to numerically increase max insulin concentrations to a small non-significant extent.
Sitagliptin alone and all sitagliptin+DXM doses significantly raised max insulin levels, but the combination of 90 mg DXM plus sitagliptin resulted in significantly higher insulin than sitagliptin alone.
All combination doses raised the baseline-adjusted AUC for insulin during the first 30 min of the test vs. sitagliptin alone.
Increase was significant for the 30 and 60 mg DXM combinations.
Sitagliptin alone led to a first 30 min AUC increase of 50%, compared with around 110% with the combination of DXM 30 or 60 mg with sitagliptin.
Sitagliptin alone failed to produce a significant rise in first 30 min AUC insulin.
Adverse
All conditions were well-tolerated. One mild adverse event (fatigue) was seen with 60 mg or 90 mg DXM plus sitagliptin.
COI: Authors are pursuing a patent for the use of morphinan derivatives in diabetes.
(Marquard, 2015) – In vitro and animal research shows DXM and other NMDAR antagonists are useful in diabetes.
This study investigated the role of NMDARs in islets, using a genetic approach to silence and delete these receptors in insulinoma cells and in the pancreata of mice, respectively. The sites were also blocked pharmacologically in insulinoma cells, mouse and human islets, diebetic mice, and individuals with T2DM.
Results
NMDARs regulate GSIS and glucose tolerance
Deletion of Grin1 gene (encoding the necessary GluN1 subunit of NMDARs) from the pancreatic epithelium of mice was associated with a higher degree of islet GSIS than was seen for islets from control mice. Basal insulin secretion was largely unaffected.
Upon beta cell-specific Grin1 deletion, most of the encoded GluN1 protein was absent from mouse islets, indicating most of the NMDARs in islets are expressed by beta cells. Notably, Grin1 deletion in beta cells alone was sufficient for greater GSIS from knockout islets compared to control islets.
Basal blood glucose concentrations in GluN1-deficient mice were also unaffected, whereas with IP glucose tolerance testing, the mice had significantly better tolerance compared to heterozygous control litter-mates.
Compared to untreated islets, MK-801 treated mouse and human islets and rat INS1E cells showed a higher amount of GSIS without any substantial effect on basal insulin secretion.
DXM and DXO increase GSIS and glucose tolerance
DXO in mouse and human islets was able to significantly increase GSIS at 10 μM without altering basal insulin secretion.
DXM also led to greater GSIS at all glucose concentrations tested, though significant effects were only seen at 10 mM glucose and higher.
IP injection of DXO in mice led to significantly higher glucose-induced plasma insulin concentration and better glucose tolerance compared to control IP injections without DXO.
Similarly, DXM led to neither changes in basal plasma insulin nor fasting blood glucose, but led to significantly higher GSIS.
Other metabolites of DXM, namely 3-hydroxymorphinan and 3-methoxymorphinan, were also found to result in greater GSIS. Whereas levorphanol, the levorotatory isomer of DXO, was significantly less effective than DXO.
DXM and DXO enhance GSIS and glucose tolerance via NMDARs
IP injection of DXO or DXM was associated with significantly better glucose tolerance in control littermates compared to the same mice without DXO/DXM. Whereas there was not a difference in mice lacking pancreatic NMDARs.
DXO requires pancreatic NMDARs for insulin secretion in vitro and in vivo.
Antidiabetic, islet cell protective effects of DXM
DXM was tested in an animal model of T2DM to see if long-term exposure was positive or negative for cell health and glucose control.
DXM was added to the drinking water of leptin receptor-deficient mice that developed T2DM within the first 1-2 months of age.
Treatment of mice with 3 mg/mL DXM for three weeks resulted in significantly lower fasting blood glucose compared with 1 mg/mL. Notably, mice treated with either concentration of DXM did not differ in their plasma levels of corticosterone, a hormone known to increase blood glucose.
At 12 weeks of age, mice receiving 3 mg/mL had better glucose tolerance and fasting blood glucose compared to those receiving 1 mg/mL.
Islet insulin content was significantly higher with the higher dose of DXM vs. lower dose. And the areas of both the insulin-expressing beta cells and the glucagon-expressing alpha cells were more than twice as large with the higher vs. lower dose.
When staining with phospho-histone 3 (marker of cell proliferation) and cleaved caspase-3 (marker of apoptosis), there was no difference in islet cell proliferation, but the number of apoptotic cells within the pancreatic islets was lower upon treatment with the higher vs. lower dose of DXM.
DXO also significantly lowered cytokine-mediated cell death in islets from two human donors vs. islets from the same donors under conditions in which cytokines induced a more than 3 fold increase in cell death vs. no cytokine treatment.
COI: J.M., T.M. and E.L. pursue a patent application (WO 2013/029762 A1) entitled Morphinan-derivatives for treating diabetes and related disorders.
Cardiovascular Protection
A few animal and in vitro studies have found evidence of effects that could be utilized to improve the health of people with cardiovascular disease. DXM was found to reduce blood pressure and offer vascular protection alone or with amlodipine in rats with experimental hypertension (Wu, 2012). It also reduced oxdiative stress and inhibited some of the mechanisms leading to atherosclerosis (Liu, 2009 ; Jiang, 2012).
Animals
(Wu, 2012) – DXM can reduce blood pressure and enhance vascular protection in experimental hypertension in rats
Rats. Controls were compared to 18-week-old male spontaneous hypertensive rats (SHRs)
SHRs were given orally:
monotherapy DXM 1, 5, or 25 mg/kg/d
monotherapy amlodipine (AM) 1, 5 mg/kg/d
Combination therapy of DXM 1, 5, or 25 mg/kg/d with AM 1, 5 mg/kg/d
Results
Monotherapy with either AM or DXM significantly reduced SBP but not DBP. The BP was similarly reduced by DXM treatment in different doses without dose-dependent effects.
Combination therapy in various doses had synergistic effects on SBP, DBP, and MBP reduction. The high dose of AM with intermediate DXM (5 mg/kg/d) was best.
Effects on vascular reactivity
Combared to control, DXM monotherapy at various doses yielded increases in both endothelium-dependent and -independent vasodilation in the aorta of SHRs. While such effects were no seen with AM monotherapy in different doses.
Effects on aortic media thickness/area
AM monotherapy did not reduce media thickness/media, but low and intermediate DXM monotherapy significantly reduced aortic media thickness/area.
Among combinations, the most effective was low dose AM with low dose DXM.
Effects on plasma total antioxidant status, nitrite/nitrate levels, and renin-angiotensis-aldosterone system
AM or DXM significantly increased TAO. While DXM monotherapy did not change plasma NOx level, AM monotherapy did significantly reduce the level as compared to no treatment. There was no change in NOx level with combination treatment.
Therefore, the combination of drugs, except with high doses, may increase plasma TAO without alteration of plasma NOx level. The combination of high dose DXM and high dose AM had no effects on either.
In the RAA system, serum renin level could be reduced via monotherapy with low dose DXM or different doses of AM, but may be increased by high dose combination of both drugs.
Serum angiotensin 2 level was increased by all treatments other than DXM high dose monotherapy and the combination of low dose DXM with AM.
Serum aldosterone was increased only by the combination of low dose DXM and high dose AM, suggesting the antihypertensive effect may be coming from an effect independent of RAA.
Effect in vitro on angiotensin II-induced ROS formation and NADPH oxidase activity in HAECs
DXM 100 μM/L for 24 hours did not impair HAECs. Compared with control, angiotensin II significantly increased ROS production of HAECs, which could be prevented by DXM treatment.
Besides, the NADPH oxidase activity of HAECs was significantly increased by angiotensin II which could be abolished by pretreatment with DXM.
COI: Not reported
(Liu, 2009) – DXM reduces oxidative stress and inhibits atherosclerosis and neointima formation in mice
In vitro and in vivo study. Cells were stressed via LPS exposure.
Results
DXM significantly suppressed production of TNF-α, monocyte chemoattractant protein-1, IL-6, IL-10, and superoxide in macrophage cell culture after LPS stimulation.
DXM reduced macrophage nicotinamide adenine dinucleotide phosphate oxidase activity via decreased membrane translocation of p47phox and p67phox via inhibition of PKC and extracellular signal-regulated kinase activation dose-dependently at either 1 μM or 1 nM in the THP-1 cell culture.
PKC and ER1/2 are essential for the phosphorylation and translocation of p47phox and p67phox to plasma membrane. Pretreatment directly reduced PKC-δ and ERK1/2 activities that were otherwise elevated by LPS.
Animal model (mice)
Anti-atherosclerotic effect was tested in two animal models: apoE-deficient mice and mouse carotid ligation model.
DXM 10-40 mg/kg/d for 10 weeks in apoE-deficient mice significantly lowered superoxide production in their polymorphonuclear leukocytes and aortas.
5 mg/kg/d had no significant effect.
DXM significantly decreased the severity of aortic atherosclerosis in the apoE-deficient mice and decreased carotid neointima formation after ligation.
COI: None. Supported by the National Science Council in Taiwan.
In vitro/Ex vivo
(Jiang, 2012) – DXM is protective against LPS-induced adhesion molecule expression to human endothelial cells, which could make it protective against atherosclerosis
This study was in vitro and ex vivo using human cell types
Results
HUVECs were pretreated with DXM for one hour, which resulted in a significant decline in LPS-induced monocyte adhesion to endothelial cells.
LPS showed an increase in monocyte adhesion and migration across the endothelium vs. the migration seen without LPS. In contrast, the ability of THP-1 cells to migrate across HUVECs was significantly decreased to 90% by the presence of DXM in a dose-dependent manner. These results show DXM can inhibit monocytic migration induced by inflammation.
LPS and and the pro-inflammatory cytokine TNF-α increased cellular levels of ICAM-1 and VCAM-1 in HUVECs. ICAM-1 expression was declined within 6 hours of exposure to DXM and VCAM-1 expression was decreased after 24 hours of exposure.
LPS clearly stimulated a rise in the level of ERK and Akt activation in HUVECs. DXM treatment resulted in an inhibition of LPS-induced ERK and Akt phosphorylation in a dose-dependent manner at 30 minutes.
COI: None
Countering Physical Dependence to Other Drugs
NMDAR antagonists have been hypothesized to offer tolerance-reducing and tolerance-preventing effects for other drugs, most often opioids. Little clinical evidence supports this efficacy in humans, though there is substantial animal evidence showing DXM and similar drugs can slow the development of tolerance and even reverse it.
It had no significant impact on methadone tolerance in a DBRCT of 72 people undergoing methadone maintenance treatment (Salehi, 2011) It failed to reduce ethanol withdrawal symptoms at 360 mg per day (Huang, 2014) and it did not improve naloxone-precipitated withdrawal symptoms in 11 people stabilized on methadone (Rosen, 1996).
DXM does appear safe when combined with methadone, however, even when it is given at 480 mg/d (Cornish, 2002). That dose produced no clinically significant vital sign changes and no serious side effects.
There is some evidence supporting its usefulness in acute opioid withdrawal. It’s effective at further reducing opioid withdrawal symptoms when added to clonidine, clonazepam, and paracetamol (Malek, 2013). Koyuncuoglu (1990) indicated it may be helpful in heroin withdrawal, but because the study was uncontrolled and involved multiple other drugs, the results cannot be easily interpreted.
A 6-day DBRCT of 65 heroin-dependent patients found 240 mg/d of DXM could improve some withdrawal symptoms from Day 3 to Day 6, but it did not change the need for other medications or improve patient’s treatment satisfaction (Lin, 2014).
Larger effects have been reported in animals. DXM at 30 mg/kg SC was able to prevent a 5-fold rise in morphine ED50 over the course of four days (Elliott, 1994). And it also successfully reversed morphine tolerance to nearly the control value when given after four days of morphine exposure. Substantial dose-dependent benefits were also seen in reducing ethanol withdrawal symptoms in rats (Erden, 1999).
Human
Effective
(Lin, 2014) – It appears to improve heroin withdrawal severity, but not substantially or during the entire time course
6-day DBRCT. DXM 240 mg/d for much of the trial. 65 subjects.
DXM group had better outcome after 3 days of treatment, with significant between-group differences for Days 3 to 6.
But the use of ancillary medications did not differ and CGI scores at discharge were not significantly different, nor was patient’s impression of treatment satisfaction. So the impact is pretty minimal at best.
COI: None
(Malek, 2013) – DXM, when combined with other treatments, does improve withdrawal symptoms from opioid dependence
DBRCT. 60 patients.
Groups:
Clonidine, clonazepam, and paracetamol.
Clonidine, clonazepam, paracetamol, and DXM 75 mg every six hours.
DXM group had milder withdrawal symptoms, mainly at the 48 and 72 hour time points.
COI: None
(Koyuncuoglu, 1990) – It can reduce opioid withdrawal symptoms when given alongside other drugs. The study involved other drugs and an uncontrolled setting, so it’s unclear what to make of the results.
56 people addicted to heroin. They were given DXM 15 mg every hour + 25 or 50 mg chlorpromazine every 6 hours.
They also received diazepam and hyoscine butylbromide and dipyrone
By the fourth day most patients felt “extremely well.”
COI: Not reported
(Cornish, 2002) – DXM is safe when combined with methadone, even at high doses.
Randomized, double-blind study investigating the safety of DXM when combined with methadone in inpatient, opioid-dependent individuals. Males receiving 50-70 mg/d methadone were included and randomized to placebo or DXM.
12-day active medication phase with patients receiving 120, 240, or 480 mg/d in increasing order (4 days each).
Results
DXM led to mild non-clinically significant elevations in heart rate, BP, temperature, and plasma bromide level.
Participants had far more adverse events (173 with DXM compared to 21 with placebo) but they were not clinically serious and the most common ones were sleepiness and drowsiness.
COI: This study was supported by an interagency agreement between NIDA, the Philadelphia Veteran’s Affairs Medical Center, and ENDO Pharmaceuticals, Inc. Support was also provided by NIDA Center Grant #P60-DA-05186.
Ineffective
(Huang, 2014) – Failure to reduce alcohol withdrawal symptoms
360 mg or placebo daily for 7 days. 40 people. No reduced need for lorazepam, indicating no improvement of alcohol withdrawal symptoms.
COI: None
(Salehi, 2011) – No significant impact on methadone tolerance in methadone maintenance
Double-blind, randomized, controlled trial. Inclusion criteria: opium addiction, age of 20-60 years, and being a good candidate for methadone maintenance.
Active group started with DXM 60 mg/d for 4 days, then it was increased to 120 mg/d (60 mg BID) for 4 days. Then during a third 4-day period it was increased to 240 mg/d (120 mg BID) which was continued for 6 weeks.
72 total participants completed all of the follow-up stages.
Results
Mean methadone consumption was 62.7 mg/d in the DXM group and 70.4 mg/d in the placebo group. This wasn’t significantly different. And no significant differences were found at any time point.
After 6 weeks of follow-up, the difference of SOWS (Short Opioid Withdrawal Scale) weren’t significantly different at 9.2 for DXM and 12.1 for placebo. The most frequent symptom was yawning in both groups. No significant differences between groups for any withdrawal symptom.
Quality of life scores didn’t significantly vary at 84.8 for DXM vs. 77.8 for placebo. Neither the difference between the groups nor the trend of QOL change was significant.
COI: None.
(Rosen, 1996) – A pilot study examining the effect of DXM in naloxone-precipitated withdrawal. Failed to significantly improve any symptoms.
11 people stabilized on methadone. Challenged with naloxone. DBRCT. DXM at 60, 120, or 240 mg. Failed to significantly attenuate any withdrawal symptoms.
COI: Study supported by NIDA.
Animal
(Yeh, 2002) – Reduction in morphine withdrawal syndrome in neonatal rats passively exposed to morphine
DXM given at 2, 5, 10, or 20 mg/kg SC. 30 minutes before naloxone.
DXM at 10 mg/kg reduced symptoms, sometimes to control level. 5 mg/kg was also effective for some symptoms.
COI: Study was supported by a grant from National Health Research Institute in Taipei, Taiwan.
(Erden, 1999) – DXM reduces withdrawal symptoms from ethanol in rats
DXM 10, 20, or 40 mg/kg IP starting in the third hour of ethanol withdrawal.
DXM dose-dependently countered withdrawal symptoms. And it significantly reduced audiogenic seizure occurrence
Rate of seizure was 80% in control vs. 50% with 10 mg/kg, 36% with 20 mg/kg, and 9% with 40 mg/kg
COI: Supported by a grant at the Kocaeli University.
(Elliott, 1994) – DXM prevents and reverses morphine tolerance in mice
Mice were given morphine and DXM. Their analgesic dose-response curves were generated from a tail-flick test.
Three tests
Test 1
DXM 30 mg/kg SC given 30 minutes prior to every morphine dose. Day 1 – Morphine 10 mg/kg SC three times daily, then 20 mg/kg on Day 2 and 40 mg/kg three times daily on Day 3.
Test 2
7-day infusion of morphine via osmotic pump. This was accompanied by either another osmotic pump with DXM or by sham surgery.
Test 3
Tolerance produced by two 25 mg morphine pellets implantated on Day 1. Cumulative dose-response study on Day 4 determined tolerance level. Then pellets were removed from tolerant mice and the mice received either DXM 30 mg/kg three times daily SC or control on Days 5, 6,7, with second cumulative dose-response test on Day 8.
Results
Test 1
DXM prevented a 5-fold rise in morphine ED50 on Day 4.
Test 2
DXM 12 mg/kg/day via SC infusion concurrently with morphine 30 mg/kg/d SC infusion prevented a 6-fold rise in morphine ED50.
Test 3
Implantation of morphine pellets (2x 25 mg) caused a 10-fold rise in morphine ED50 on Day 4. DXM 30 mg/kg SC three times daily reversed morphine tolerance with a near return to the control value.
DXM 1 or 2 mg/kg IP given prior to naloxone. 1 mg/kg significantly attenuated symptoms and 2 mg/kg led to attenuation or prevention of all withdrawal signs.
COI: Not reported
Addiction
DXM may reduce psychological dependence even if it doesn’t improve physical dependence. Lee (2015) found 60 mg of sustained release DXM significantly reduced the concomitant use of illicit opioids by methadone maintenance patients, but it did not change how much methadone they required. Oddly, this benefit was not seen with 120 mg DXM.
Animal studies have consistently found DXM and DXO can reduce the rewarding properties of drugs, reduce psychological dependence (as shown by tests like the conditioned place preference test), and perhaps reduce behavioral sensitization. This has been shown for opioids, methamphetamine, and nicotine (Briggs, 2016 ; Yang, 2012 ; Chen, 2011 ; Lue, 2007 ; Huang, 2003).
Co-administering 10 mg/kg IP of DXM with morphine can block a morphine-induced rise in extracellular dopamine levels (Huang, 2003). Its beneficial properties have been linked to the nucleus accumbens (NAc) and ventral tegmental area (VTA), since injecting it directly into those brain regions can also counter signs of psychological dependence (Lue, 2007).
Chen (2011) found evidence for a role of σ1 receptors, since blocking that site attenuated DXM’s ability to reduce the rewarding nature of morphine.
Humans
(Lee, 2015) – DXM may reduce drug-seeking in methadone maintenance therapy.
Participants were placed into groups:
Methadone + placebo
Methadone + one daily dose of 60 mg DXM sustained release
Methadone + one daily dose of 120 mg DXM sustained release
The primary outcome was to compare the dose of methadone required, retention rates, and concomitant opioid use measured by plasma morphine levels.
196 opioid-dependent participants were included in the 12-week trial.
Results
By the end of the double-blind phase, 68.4% of participants remained. The dropouts were distributed almost evenly across groups, though they were a little higher in the placebo group.
Methadone dose
The changes in the required methadone dose were not significantly different.
Plasma morphine/Concomitant drug use
Plasma morphine was significantly lower in the DXM 60 mg group (p=0.003) but not the DXM 120 mg group, compared with placebo.
The DXM 120 mg group’s plasma morphine did not significantly change at all, but the placebo group had a significant trend of increasing plasma morphine levels, while the DXM 60 mg group had a significant trend of decreasing plasma morphine.
Other
DXM 60 mg group had a significantly (p=0.049) lower TNF-α level than placebo, but other cytokine and BDNF levels were not significantly altered.
When correcting for multiple comparisons with a significance value of p<0.025, it was not significant.
There was no significant difference between placebo and 120 mg DXM.
Retention was significantly higher in the 60 mg group than in the placebo group, with no significant benefit to 120 mg DXM.
COI: None
Animals
(Briggs, 2016) – DXM interacts with serotonergic and histaminergic targets to reduce nicotine self-administration
Rats. Trained to self-administer nicotine. DXM was given 10 minutes before sessions.
Results
Study 1
DXM at 10 mg/kg, and more so at 30 mg/kg, significantly decreased locomotor activity.
Acute DXM caused a dose-related decline in nicotine self-administration.
There was a threshold between 3 and 10 mg/kg for significantly reducing administration.
The impact on nicotine responding was much greater than with food responding. 30 mg/kg only decreased food responding to 89%, while it decreased nicotine administration to 39.6%.
Study 2
Pyrilamine (antihistamine) significantly augmented 10 mg/kg and 30 mg/kg DXM. When pyrilamine was present, those doses produced a significantly greater reduction in locomotor activity.
Mepyramine 13.3 mg/kg significantly reduced nicotine administration relative to control. And the combo of DXM 10 mg/kg and mepyramine 13.3 mg/kg significantly lowered administration more than either drug alone.
Study 3
Lorcaserin (5-HT2C agonist) 0.3125 mg/kg significantly interacted with 10 mg/kg DXM in reducing administration more than if either drug was used alone. Whereas no significant interaction was seen for food self-administration.
Both drugs significantly decreased nicotine self-administration dose-dependently. 10 mg/kg DXM with 0.3125 mg/kg lorcaserin reduced nicotine self-administration significantly more than either drug alone.
COI: Not reported
(Yang, 2012) – Protective, even when give post-administration, against drug-seeking and behavioral sensitization induced by methamphetamine
Rats given methamphetamine (1 mg/kg IP once daily), DXM (20 mg/kg IP twice daily)
Turnover rates of dopamine calculated based on (DOPAC+HVA)/DA
Results
Results
Methamphetamine has rewarding effects
Even by Day 13 (after methamphetamine had been stopped through Days 8-12) the rats still showed significant CPP, indicating maintenance of drug-seeking.
DXM completely abolished the rise in CPP when given for 4 days from Day 9-12
Methamphetamine caused behavioral sensitization
It both acutely and post-treatment led to a rise in ambulatory locomotor activity and total locomotor activity, with the rise in activity after a single methamphetamine dose on Day 13 being significantly higher than on Day 1.
When DXM was given for 4 days, it led to methamphetamine only producing a Day 1-level increase in locomotor activity, indicating a lack of expression of sensitization.
By itself, DXM had no rewarding or behavioral sensitization effect
Investigating the relevant brain regions
DXM (0.1 nM) microinjected into either the NAc shell or VTA twice daily for 4 days during methamphetamine withdrawal was able to completely reverse meth-induced CPP, indicating DXM acts at both to inhibit the drug-seeking.
Whereas behavioral sensitization was only blocked if DXM was given into the VTA.
DA turnover
DA turnover rate in the NAc and mPFC was significantly increased by acute and chronic methamphetamine treatment.
The turnover rate was significantly reduced in the mPFC by DXM, not differing from the control group.
If DXM was given into the NAc, it could block the methamphetamine-induced rise in DA turnover rate in both the NAc and mPFC.
COI: National Science Council, Taiwan; Contract grant number: NSC 93-2320-B-016-033; Contract grant sponsor: Department of Health, Taiwan; Contract grant number: DOH94-NNB-1034; Contract grant sponsor: Department of Defense, Taiwan; Contract grant number: DOD97-09-01; Contract grant sponsor: National Health Research Institutes, Taiwan; Contract grant number: NHRI-99A1-PDCO-0809111
(Chen, 2011) – Very low doses of DXM can attenuate morphine’s rewarding effects via a σ1 route
Conditioned place preference test. And a locomotor activity test to look for behavioral sensitization.
Rats exposed to the treatment conditions for six days.
Results
DXM (3 or 10 μg/kg IP) was co-administered with morphine (5 mg/kg SC) and effectively blocked its rewarding effect, but not behavioral sensitization.
This inhibiting effect of DXM was removed if the σ1 antagonist BD1047 (3 mg/kg IP) was also given.
And when BD1047 (5 nM) was locally administered to the VTA, the efficacy of DXM was also blocked.
COI: None
(Lue, 2007) – DXM reverses drug-seeking but not behavioral sensitization when given after subchronic morphine
Rats given morphine (5 mg/kg IP once in the afternoon); DXM (20 mg/kg IP twice per day).
CPP test over 16 days
Results
After 4 days of withdrawal from morphine, rats still showed significant CPP. Treatment with DXM during those 4 days abolished the CPP.
Acute morphine didn’t affect locomotor activity of rats, but both ambulatory activity and total activity were significantly greater on Day 13 after a single morphine dose vs. on Day 1, showing sensitization.
DXM failed to prevent the expression of this sensitization.
Acute morphine increased DA turnover significantly only in the NAc, not the DS or mPFC.
A single injection of morphine after subchronic morphine and withdrawal for 5 days increased turnover further in the NAc and also increased it in the DS and mPFC.
DXM treatment for 4 days reversed the subchronic effect of morphine in the NAc but not the DS or mPFC.
Investigating the brain regions
DXM (0.1 nM) microinjected into the NAc shell or VTA twice daily for 4 days during withdrawal completely reversed morphine-induced CPP.
COI: National Health Research Institutes; Contract grant number: NHRI-EX94-9401NP; Contract grant sponsor: National Science Council; Contract grant number: NSC 93-NU-7-016-001; Contract grant sponsor: C.Y. Chai Foundation for the Advancement of Education, Science and Medicine, Taiwan, Republic of China.
Either morphine (10 mg/kg IP) or morphine along with DXM (10 mg/kg IP).
Results
DXM itself led to no rewarding effect on the CPP test. While morphine given four times over 8 days led to marked place preference. DXM co-administration abolished the rewarding effect of morphine.
DXM was unable to block behavioral sensitization induced by morphine. Morphine rats showed a significant rise in locomotor activity, which was also higher in those receiving DXM with morphine.
DXM itself did not show any impact on activity.
DXM itself had no impact on extracellular levels of DOPAC or HVA (dopamine metabolites). But morphine significantly raised the extracellular levels of DOPAC and HVA in the shell region of the NAc.
Co-administration of DXM reversed the effect of morphine.
Though it wasn’t significant, morphine also seemed to raise the extracellular level of the serotonin metabolite 5-HIAA, which was also blocked by DXM.
COI: This study was supported by grants from the National Health Research Institutes (NHRI-EX91-8909BP), and the National Science Council (NSC 90-2320-B-016-034), Taipei, Taiwan.
(Glick, 2001) – It can block the self-administration of morphine, methamphetamine, and nicotine. Study also shows equipotency with dextrorphan.
Rats
Experiments with DXM and DXO were conducted after self-administration was stabilized, typically after 2 weeks of testing.
Both DXM and DXO decreased morphine self-administration at 10-30 mg/kg SC, methamphetamine at 20 and 30 mg/kg SC, and nicotine at 5-30 mg/kg SC.
In both cases, under 40 mg/kg wasn’t able to affect responding for water.
The equal potencies of DXM and DXO suggest mediation of the effects by a non-NMDA receptor target, possibly antagonism of α3β4 nicotinic receptors, for which the two drugs have a closer potency.
COI: This study was supported by NIDA grant DA 03817.
(Kim, 2001) – It affects cocaine-mediated behavioral effects along with producing a long-lasting Fos-related immunoreactivity difference
Studied in mice
DXM (40 mg/kg IP) decreases locomotor activity caused by high doses of cocaine (20 mg/kg IP), but it does not affect hyperactivity from 10 mg/kg cocaine, while it increases locomotor activity from 5 mg/kg IP.
Repeated administration with cocaine or DXM also increases FRA-immunoreactivity in the nucleus accumbens and striatum that lasted at least 7 days.
DXM (40 mg/kg IP) significantly increased FRA-immunoreactivity induced by 5 mg/kg cocaine while significantly decreasing the FRA-immunoreactivity caused by cocaine 20 mg/kg.
COI: This study was supported by BK project and a grant (# HMP-99-N-02-0003) of the Good Health Research and Development Project (1999) of the Ministry of Health and Welfare, Republic of Korea. We thank Drs. J.S. Hong and M.J. Iadarola for donating antiserum against FRA.
Allowed to self-administer methamphetamine in 2-hour sessions, 5-7 days/week. All were initially trained on 0.1 mg/kg (IV) methamphetamine, with a correct response in the nose poke producing an injection.
After this, methamphetamine was replaced with vehicle for five consecutive sessions. Then the rats went split into three groups of 5:
1. Allowed to self-administer 0.05 mg/kg methamphetamine
2. Allowed to self-administer 0.1 mg/kg methamphetamine
3. Allowed to self-administer 0.25 mg/kg methamphetamine
These rats were stabilized for five consecutive sessions, then testing was conducted on 5 more consecutive test days with DXM pretreatment, with the animals receiving DXM (25 mg/kg IP) immediately before the start of each session.
Results
It took 14-21 sessions for all animals to consistently self-administer the training dose of 0.1 mg/kg methamphetamine. Analysis showed that during the methamphetamine trials, animals responded significantly more often in the correct than incorrect hole. Responding declined when saline was substituted for methamphetamine.
DXM significantly reduced self-administration at all three methamphetamine doses. But no significant suppression was seen when testing DXM’s effect on food responding.
COI: NIDA Intramural Research Funds supported the research
Rats trained on IV cocaine (0.25 mg/injection) until stable drug intake for 3 days was reached.
Then pretreated with DXM (10, 25, 50 mg/kg IP) immediately before the cocaine administration session; each dose tested only once for each animal.
Results
DXM significantly reduced cocaine self-administration during all time intervals considered, although more effectively during the first 30 min. Significance at all doses of DXM during the first 60 min of the session was seen.
DXM significantly reduced responding for cocaine and pretreatment with 25 mg/kg significantly reduced the maximum responding for cocaine self-administration.
COI: This is manuscript number 10201-NP of The Scripps Research Insitute. This work was partially supported by NIDA grants DA 04398. L.P. is a recipient of a Fellowship from the ‘C. Mondino’ Foundation
Cough
DXM is a very popular cough medication, but although some evidence suggests it could work, it is similar to codeine in that for most people DXM probably is not going to substantially improve their symptoms.
Most studies have found that in children and adults with an upper respiratory infection (URTI), symptoms are not significantly improved by DXM at its standard dose of ~30 mg for adults and less for children (Paul, 2004 ; Schroeder, 2002 ; Lee, 2000). It also wasn’t effective in smoking-related cough at 30 mg (Ramsay, 2008).
Some studies show an effect, though it is pretty negligible. Paul (2007) found honey was significantly superior to placebo, while DXM wasn’t. At the same time, honey was not significantly superior to DXM, indicating how small the effect size is for either treatment. Unlike Paul (2007), a separate study of young children with URTI-related cough found DXM 7.5 mg, diphenhydrameine (DPH) 6.25 mg, and honey were all significantly better than placebo, though with honey coming out on top.
DXM has most reliably shown an effect in induced cough, such as from citric acid, fentanyl injection, and capsaicin (Faruqi, 2014 ; Marashi, 2013 ; Elmenesy, 2011 ; Grattan, 1995). Indeed, Ramsay (2008) failed to show a benefit in smoking-related cough, while also showing DXM did have an effect in a citric acid test. Different coughs are amenable to different treatments.
The benefits in citric acid-induced cough seem to be reliant on DXM itself, not a metabolite. An otherwise ineffective dose of 30 mg can become effective once CYP2D6 is inhibited with quinidine (Manap, 1999).
Some efficacy has been shown in persistent cough, albeit in an uncontrolled setting (Donno, 1994) and it was more effective than codeine in chronic cough from pulmonary tuberculosis, bronchial carcinoma, or obstructive lung disease (Matthys, 1983).
Effective
(Robertson, 2016) – The evidence is mixed for DXM reducing URTI cough, but some studies do indicate some benefit beyond placebo
A 2014 systematic review of 10 trials in children and adults, involving DXM in 4 studies, antihistamines in 3 studies, letosteine in 1 study, and antihistamine/decongestant in 1 study.
No difference in cough relief by child- or parent-reported symptom scores or sleep duration with these medications vs. placebo.
A report of 3 RCTs (n=451 adults)
DXM decreased mean recorded cough count by 19% to 36% compared to placebo.
Meta-analysis of 5 RCTs (n=710)
DXM decreased cough bouts, cough effort, and cough latency by 12% to 17% vs. placebo
COI: Not reported
(Faruqi, 2014) – DXM, but not butamirate, is significantly effective in capsaicin induced cough
34 subjects. DXM 30 mg oral. DXM was superior to placebo (p=0.01) for increasing the concentration of capsaicin eliciting 5 or more coughs in 15 sec. Though it didn’t have a significant effect on the secondary endpoint, which looked at the concentration of capsaicin producing 2 or more coughs.
COI: This study was supported by Novartis via an unrestricted grant.
(Marashi, 2013) – DXM is effective in reducing fentanyl-induced cough
360 adults. Comparing clonidine to DXM 15 mg oral before surgery. 20% of patients had cough attacks classified as fentanyl-induced. Overall incidence similar between DXM and clonidine, but significantly superior to placebo.
Cough severity was also significantly lower in both drug groups compared to placebo.
COI: Not reported
(Elmenesy, 2011) – DXM can improve fentanyl-induced cough frequency and severity
DXM 60 mg IV or placebo before surgery. The number of patients with fentanyl-induced coughing was 13% for DXM group and 36% for placebo. The average severity was also lower.
COI: Not reported
(Shadkam, 2010) – DXM does reduce nightly cough in children, but it’s less effective than honey.
139 children aged 24-60 months. URTI-related cough. 7.5 mg DXM vs. 6.25 mg DPH vs. 2.5 mL local honey vs. placebo
Honey was significantly superior to all other groups. DXM and DPH were significantly superior to placebo, though the difference between the two of them was not. All p<0.001
COI: None. The study was funded by the Shahid Sadoughi University of Medical Sciences.
(Manap, 1999) – DXM significantly lowers induced cough and the effect is greater with CYP2D6 inhibition
22 healthy extensive metabolizers at CYP2D6.
Citric acid test
Significantly greater antitussive effect from DXM 60 mg vs. placebo and DXM 30 mg+quinidine vs. placebo, while DXM 30 mg on its own was not effective. Therefore, an otherwise ineffective dose could become effective with CYP2D6 inhibition.
COI: Not reported
(Grattan, 1995) – Efficacy demonstrated for citric acid-induced cough
Oral DXM 30 mg had a significant effect, but inhaled DXM did not.
COI: Supported in some way by SmithKline Beecham.
(Donno, 1994) – DXM appears effective in persistent cough, though the study was not placebo-controlled.
Moguisteine vs. DXM. 124 adults with persistent cough, often from obstructive chronic bronchitis. DXM given 3 times over a 2 day period at 30 mg per dose.
For both drugs there was a significant reduction in cough number and subjective cough frequency and cough troublesomeness. There was little difference between groups.
COI: Supported by Boehringer Mannheim
(Matthys, 1983) – DXM is more effective than codeine and placebo in chronic cough
16 patients with chronic cough from pulmonary tuberculosis, bronchial carcinoma, or obstructive lung disease
Each patient given two doses of 20 mg DXM, 20 mg codeine, or placebo for three consecutive nights.
DXM suppressed cough frequency more than codeine (number of coughs per hour): 5.6 DXM, 5.8 codeine, 9.6 placebo.
Cough intensity was significantly lower. DXM and codeine were similar in the first three hours, but then DXM was more effective. And the overall difference between them was significant.
DXM was significantly better than the others based on subjective reports of the most effective drug, which allowed unbroken sleep, and which caused the least side effects
COI: Not reported
Ineffective
(Ramsay, 2008) – DXM is not significantly better than placebo in smoking-related cough.
42 people. Optimized oral cough formulation of DXM equivalent to 30 mg.
No significant difference in daytime or nighttime daily cough symptoms vs. placebo. Yet in a citric acid cough test, DXM was significantly superior to placebo.
COI: Author is an employee of Procter & Gamble Company.
(Paul, 2007) – Compared to placebo and DXM, honey is more effective for cough in children with acute URTI, though honey and DXM aren’t significantly different.
105 children with URTI-related acute nocturnal cough. DXM dose of 8.5 to 34 mg depending on age.
Honey was consistently best and was significantly superior to placebo. DXM was not significantly superior to placebo, though honey was not significantly superior to DXM.
COI: Supported by an unrestricted research grant from the National Honey Board, an industry-funded agency of the US Department of Agriculture.
(Paul, 2004) – No significant effect on cough in children with URTI
100 children. URTI and nocturnal cough. 7.5-30 mg depending on age. Compared to DPH (1.25 mg/kg with a max of 50 mg) and placebo.
All groups had significant improvements after treatment, but neither diphenhydramine nor DXM was significantly more effective than placebo, according to patients and parents.
COI: The study was supported by funds from the Children’s Miracle Network.
(Schroeder, 2002) – Review of its effects in acute cough in children. OTC medications, including DXM, do not appear effective.
Children and adolescents. Acute cough from URTI. 6 trials covering 438 patients.
No good evidence for or against the efficacy of DXM, codeine, mucolytics, or antihistamines in URTI-related cough in young people. Typically both drugs and placebo produce significant declines in coughing.
COI: Funded by the Division of Primary Health Care, University of Bristol and by the South & West Research and Development Directorate.
(Lee, 2000) – No significant effect on cough in URTI.
30 mg. 43 patients randomized to placebo or DXM. Similar significant trends for both groups in cough measures, but little difference between the groups.
COI: Not reported
Bipolar Disorder
Studies have not shown DXM is generally beneficial in bipolar disorder, but it may be helpful in subsets of patients with genetic polymorphisms that produce lower COMT enzyme activity (Lee, 2017) or lower levels of dopamine D2 receptors (Lee, 2012). It could assist with lowering inflammatory cytokines or raising BDNF, two factors that might contribute to bipolar symptoms.
A double-blind controlled trial of 309 patients failed to show a benefit of adding DXM 60 mg to valproate treatment, but DXM treatment did lead to higher BDNF levels.
Effective
(Lee, 2017) – DXM is effective at reducing depression symptoms in bipolar patients with COMT Val158Met polymorphism
Background
The gene encoding for COMT can undergo a polymorphism that causes an amino acid shift from valine to methionine. The Met allele encodes for enzyme activity that is 3-4x lower than normal. Low-activity allele status may increase susceptibility to bipolar disorder and it is proposed that COMT enzyme activity status may be related to the treatment response of bipolar because the COMT gene also affects response to mood stabilizers and antidepressants.
Randomized, double-blind, controlled 12-week trial of add-on DXM to valproate.
Assigned to placebo or DXM 30 or 60 mg/d.
309 patients recruited and randomized. 64.1% completed the double-blind phase.
Results
Genotype distributions of the COMT Val158Met polymorphism in groups
Distributions of the COMT Val158Met polymorphism and the baseline HDRS and YMRS scores were similar at baseline between the groups.
COMT Val158Met polymorphism was significantly associated with the changes in HDRS score.
The COMT polymorphism was not associated with YMRS (mania symptom) response.
After stratifying patients by genotype, those with the polymorphism showed a significant association between 30 mg of add-on DXM and their decline in HDRS score.
COI: None
(Kelly, 2014) – Possible improvement from DXM added to existing bipolar treatment, though it produced a high dropout rate
Retrospective chart review of patients with resistant bipolar II or bipolar NOS disorder. They received DXM 20 mg and quinidine 10 mg oral once or twice daily.
Primary outcome measure: CGI-I score after 90 days of treatment.
58 patients examined
Results
Some patients began reporting improvement within 1-2 days of starting the combo.
19 patients discontinued due to adverse effects, chiefly nausea.
3 patients had worsening of bipolar symptoms: 2 were more irritable and 1 had a rise in racing thoughts. The worsening was not massive, with a CGI-I change of -1. The symptoms resolved within 1-2 days of stopping the combination.
The combination was stopped in 11 more patients due to lack of improvement. All had reached twice daily dosing.
3 who had a favorable response with +2 on CGI-I, yet still discontinued it, then reported a worsening of symptoms of depression. The worsening resolved soon after starting the combo again.
COI: Study was entirely self-funded.
(Lee, 2012) – The DRD2/ANKK1 gene is associated with the response of bipolar disorder to DXM
Background
The DRD2/ANKK1 Taq-IA restriction fragment length polymorphism is associated with density of DRD2. DRD2 density is 30-40% lower in A1 allele carriers vs homozygotic A2 allele carriers. And this polymorphism may also be associated with mood disorder.
250 bipolar disorder patients were studied. 12-week study.
Groups
DXM 60 mg/d or placebo in addition to continuing open-label valproate that had started before the study began, making DXM an add-on treatment.
Results
YMRS and HDRS scores significantly decreased by Week 12 in all groups with no significant difference betwen groups.
The DRD2/ANKK1 TaqIA polymorphism was significantly associated with YMRS change in the DXM groups. There was a significant association between add-on DXM and decreases in YMRS score in the A1/A1 genotype.
COI: None. This work was supported in part by grant NSC98-2314-B-006-022-MY3 (to RBL) from the Taiwan National Science Council, grant DOH 95-TD-M-113-055 (to RBL) from the Taiwan Department of Health, grant NHRI-EX-97-9738NI (to RBL) from the Taiwan National Health Research Institute, and the National Cheng Kung University Project for Promoting Academic Excellence and Developing World Class Research Centers.
Ineffective
(Chen, 2014) – It is not beneficial in conjunction with valproate treatment for Bipolar disorder
Study evaluated whether DXM adds to the efficacy of valproate.
309 patients and 123 healthy controls.
Patients underwent one week of open-label valproate only at 500-1000 mg/d. Then they were randomly assigned to placebo+valproate, or valproate with DXM 30 mg/d oral, or valproate with DXM 60 mg/d oral.
They received those treatments as part of a 12-week double-blind trial.
Results
Before treatment, patients had significantly higher plasma TNF-α (p=0.025) and IL-8 (p<0.0001) levels. They also had lower plasma BDNF levels vs healthy controls (p=0.033).
Of the 309 patients who enrolled, 64.1% completed the double-blind phase. The dropout rate was similar between valproate-only and valproate+DXM groups.
After 12 weeks, the HDRS and YMRS scores improved in all groups. Plasma TNF-α and IL-8 levels were also lower in all groups.
Significant difference (p=0.026) in plasma BDNF between the valproate+DXM60 and valproate+placebo group.
COI: None. Study was funded by the Taiwan National Science Council and National Cheng Kung University Project.
Neuroprotection
DXM reliably produces protection from neurotoxic insults in animals. The beneficial properties are seen in glutamate toxicity, endotoxin exposure, methamphetamine toxicity, MDMA toxicity, hyperoxia, and blood supply reduction (Ma 2016 ; Xu, 2016 ; Madeira, 2015 ; Posod 2014).
Some of the primary mechanisms underlying its efficacy are its inhibition of glial cell activation and its inhibition of excitotoxicity (Madeira, 2015 ; Werling, 2007). It has anti-inflammatory and antioxidant properties in the central nervous system in neurotoxic conditions. Beneficial effects are also seen with 3-hydroxymorphinan and DXO, two of its metabolites (Zhang, 2004 ; Steinberg, 1988).
It has been shown to inhibit production and secretion of inflammatory mediators like TNF-α, IL-6, and nitric oxide (Madeira, 2015).
Though it consistently has protective effects in animals and in vitro, clinical evidence of benefit is lacking. Some of the negative findings could be due to DXM not reaching the CNS at adequate concentrations. Mousavi (2010) reported no benefit other than a potential decline in post-stroke seizure rate from 300 mg/d in 40 patients with stroke. If DXM is to provide clinical benefit, it may need to be dosed at a higher level.
Steinberg (1996) gave patients 0.8 to 9.84 mg/kg and still only showed concentrations comparable to animal and in vitro studies in a minority of patients. Because the required dosing regimen is much greater than the amount used for cough and other disorders, there may be understandable hesitation about giving hundreds of milligrams to vulnerable patients, though even the highest doses in Steinberg’s paper didn’t produce severe side effects.
Human
Effective
Ineffective
(Mousavi, 2010) – DXM did not have any clear benefit on neurological function in acute stroke
40 patients with moderate acute stroke were randomized to either DXM 300 mg/d or placebo for five days.
Results
Mean stroke scores didn’t significantly differ between groups at Day 5 or at the 3-month follow up
Patients given DXM showed a significant reduction in seizures (complication post-stroke), but they had a higher chance of myocardial infarction and renal failure.
COI: Not reported
Etc
(Steinberg, 1996) – Potentially neuroprotective concentrations can be reached in humans without serious adverse effects
181 patients undergoing intracranial surgery or endovascular procedures were exposed to ascending doses of DXM prior to and 24 hours after surgery. The doses were 0.8 to 9.64 mg/kg.
Results
Concentrations
Brain levels were 68-fold higher than serum, while CSF was 4-fold lower. Max levels: 1514 ng/mL (serum), 118 ng/mL (CSF), 92,600 ng/g (brain). And for DXO: 501 ng/mL (serum), 167 ng/mL (CSF), and 6840 ng/g (brain).
For 11 patients, the brain and plasma levels were comparable to those seen in successful animal neuroprotection studies.
Side effects
At neuroprotective levels: Nystagmus (64%), nausea and vomiting (27%), distorted vision (27%), ataxia (27%), and dizziness (27%) were common. All side effects were reversible and no patient had severe adverse reactions. The side effects typically were not bothersome to patients.
Most patients had euphoria and others had visual hallucinations or persecutory delusions. Visual hallucinations tended to consist of seeing animals. 2 patients thought members of the medical team were going to harm them.
Agitation due to hallucinations caused management difficulties in a few patients.
Nausea and vomiting were easily managed with antiemetics like prochlorperazine, promethazine, or droperidol.
60-64% experienced side effects at doses over 4 mg/kg. When given 2.1 mg/kg or less, no side effects were observed.
COI: Not reported
Animal
Effective
(Ma, 2016) – DXM protects against the neurotoxic action of MDMA in primates
Examining the long-term effect of MDMA vs. MDMA + DXM on primate brain. Studying the serotonergic system using SPECT. 9 monkeys
Dosing: SC injections of DXM (5 mg/kg) and MDMA (5 mg/kg) or MDMA alone. Given twice daily for 4 consecutive days. DXM was always administered 5 minutes before MDMA.
Long-term effects evaluated via SERT imaging at 1, 4, 24, 30, 48, and 54 months.
The uptake ratios of labeled ligand at SERT was significantly lower in the brains of the MDMA vs. control group, indicating lower SERT levels after MDMA. The decrease in brain SERT could persist for over four years.
The loss of brain SERT levels was not observed in the group also receiving DXM.
COI: This work was supported by grants from the Ministry of Science and Technology (NSC 102-2623-E-016-005-NU, NSC 101-2623-E-016-002-NU and NSC 99-2314-B-016-030-MY3) and from Ministry of Defense (MAB-104-060), Taiwan.
(Xu, 2016) – DXM is protective at hippocampal neurons in a model of vascular dementia
Rats were subjected to two-vessel occlusion and randomly divided into groups
Sham group
Control with occlusion procedure
Procedure with 0.2 mg/kg DXM IP
Procedure with 2 mg/kg DXM IP
When DXM was given, it was provided 30 min after surgery and every day until the rats were euthanized.
On Day 31 post-procedure, there was a 5-day Morris Water Maze test. And on Day 37, the rats were killed.
Results
DXM attenuates neuronal loss and glial activation in the hippocampal CA1 region
The number of NeuN-positive cells was significantly reduced to 70% in the CA1 region in the rats who received the procedure. And the loss of NeuN-positive cells was mitigated by DXM 2 mg/kg.
The number of GFAP-positive astrocytes and Iba-1 microglia in the CA1 was significantly decreased after DXM.
DXM protected white matter in the striatum and optic tract area
Many neuronal fibers intensely expressed SMI-32 in the fiber fasocicles of the internal capsule of the striatum in the operated rats and a decrease of MBP was also seen. DXM 2 mg/kg ameliorated the negative effect.
Chronic cerebral hypoperfusion significantly increased microglial activation in the optic tract, which was significantly reduced by DXM 2 mg/kg. The number of Iba-1-positive microglia in the optic tract was significantly decreased to 71% vs. operation-only rats.
HO-1 plays a role in neuroprotection
DXM 2 mg/kg rats had a significantly higher level of HO-1. There was a significant increase in Nrf2 in the nucleus and a significant decline in the cytoplasm, indicating nuclear translocation of Nrf2 mediates the rise in HO-1.
The number of caspase-3-positive cells was reduced by 25% by DXM 2 mg/kg. These results are consistent with HO-1 and Nrf2 being essential for neuroprotection.
DXM 2 mg/kg decreases oxidative stress in the CA1
The activity of antioxidant enzymes like SOD was increased after DXM and the inflammation mediator level of TNF-α was significantly lower in the CA1 vs. rats not receiving DXM.
It also reduced the level of NOX-1 in the hippocampus.
DXM 2 mg/kg reduces impairments on the morris water maze
CCH from the operation resulted in significant impairment in spatial learning compared with control animals. Those receiving DXM 2 mg/kg had shorter mean latencies in locating the platform compared to the operation group and the DXM 0.2 mg/kg group.
The % of time and distance spent in the target quadrant was significantly higher in the DXM vs. operated rats.
COI: None. This research project was supported by grants from National Natural Science Foundation of China (31271125).
(Pu, 2015) – In rats, it is neuroprotective via anti-inflammatory and anti-excitotoxic properties
Traumatic brain injury was induced in rats via the controlled cortical impact (CCI) injury. Rats were split into groups: sham-operated, TBI, and DXM treatment.
DXM was given at 30 mg/kg IP immediately after injury.
Results
DXM significantly reduced the brain edema and neurological (i.e. motor) deficits seen after injury. It was associated with higher neuronal survival. There was a decline of TNF-α, IL-1β, IL-6 protein expression in the cortex and higher glutamate/aspartate and glutamate-transporter-1 levels in the cortex.
COI: Not reported
(Posod, 2014) – DXM protects in vivo and in vitro against hyperoxia-induced cell death
Background
Preterm infants are prematurely exposed to relatively hyperoxic conditions, even if supplemental oxygen is not given.
In vitro: Pre- and immature oligodendroglial (OLN-93) cells. They were exposed to hyperoxic conditions for 48 hours following dose-escalating pretreatment with DXM.
DXM was given at 1, 5, or 10 μM.
In vivo: Rat pups received a single IP injection of DXM at two doses prior to being exposed to hyperoxia for 24 hours. Cell viability and caspase-3 activation were the end parameters of interest.
DXM was given at 5 μg/g bodyweight (low-dose), 25 μg/g (high dose), or placebo.
Results
DXM significantly increased cell viability in immature OLN-93 subjected to hyperoxia. In pre-oligodendroglial cells, viability was not significantly affected.
In vivo
Caspase-3 activation from hyperoxia was significantly lower post-DXM in gray and white matter areas, indicating lower caspase-3-related cell death. High dose treatment was effective in parieto-occipital, temporo-parietal, retrosplenial cortex, as well in caudal, and rostral section plane white matter.
Effects on caspase-3 were not significant in the cingulate cortex or hippocampal dentate gyrus.
When control animals were given DXM there was no significant caspase-3 effect.
COI: None. Work supported by a grant from the Medizinischer Forschungsfonds Tirol.
(Shin, 2007) – DXM attenuates trimethyltin-induced neurotoxicity in rats via σ1 agonism
Rats given trimethyltin (8 mg/kg IP). They also received DXM (12.5 or 25 mg/kg SC) twice at an interval of 6 hours, then receiving trimethyltin 30 min after the last administration.
DXM was given once daily for 26 days following trimethyltin administration and the rats were killed 30 min post-final DXM dose.
When the antagonists were given, they were administered 15 min before every dose of DXM.
DXM attenuates trimethyltin-induced neurotoxicity, including convulsions, hippocampal degeneration, and spatial memory impairments.
These protective effects are reversed in the presence of a σ1 antagonist, but not a σ2 antagonist.
Affinity (rat brain Ki)
σ1
DXM: 142 nM
DXO: 344 nM
σ2
DXM: 16873 nM
DXO: 12987 nM
PCP NMDAR site
DXM: 8945 nM
DXO: 486 nM
COI: This study was supported by a grant of the Korea Health 21 R&D Project (A020007), Ministry of Health & welfare, Republic of Korea, by a grant (M103KV010013- 06K220201310) from the Brain Research Center from the 21st Century Frontier Research Program funded by the Ministry of Science and Technology, Republic of Korea, and by Brain Korea 21 project.
(Comi, 2006) – DXM is neuroprotective after ischemia in male, but not female mice.
CD1 mice (postnatal day 12) (n=72). They received unilateral carotid ligations, which can produce ischemic brain injury without hypoxia. Brain injury correlates with seizures in the first few hours after ligation.
After the carotid ligation, mice received DXM 30 mg/kg (SC).
Results
Brain injury in placebo animals was significantly greater than in DXM animals. But, upon separating the data by sex, a significant effect was only seen in male mice mice. In the male animals, brain injury was significantly reduced in the striatum and thalamus. Significantly more DXM-treated male mice had mild injury than saline-treated male mice.
In female mice, brain injury did not differ significantly based on vehicle or active treatment. There was also no shift towards milder injury.
In the vehicle treated animals, seizure score correlated with brain injury. The correlation could not be investigated in DXM animals because the drug produced acute behavioral effects like repeated jumping with sudden extension of limbs and frequent, prolonged loss of ambulation.
COI: Not reported
(Thomas, 2005) – DXM blocks microglial activation and protects against methamphetamine-induced neurotoxicity
BV-2 mice cells were used for in vitro tests
In vivo tests used mice
Given methamphetamine 4x at 5 mg/kg (IP) with a 2 hour interval between injections.
MK-801 (1.0 mg/kg IP) or DXM (25 mg/kg IP) were given 15 min prior to each methamphetamine injection.
Mice were killed 48 h after the last methamphetamine injection
Results
In vitro
LPS-related effects
LPS and Tat72, two microglial activators associated with microglial-mediated neuronal damage, were able to significantly increase expression of Cox-2 protein in BV-2 cells. LPS increased the level by 30-fold, which was prevented in a concentration-dependent manner by MK-801 and DXM provided substantial protection as well.
EC50 for MK-801 was 200 μM. ED50 for DXM was 80 μM.
Tat72-induced effects
Both drugs also reduced Tat72-induced rises in Cox-2. They were somewhat less potent, but still significantly effective, in this test.
Alone, neither drug altered Cox-2 expression.
TNF-α levels (activated microglia can secrete increased levels of TNF-α)
LPS
Both drugs caused concentration-dependent reductions in the effect of LPS on microglial TNF-α. EC50 of 400 μM for MK-801 and 150 μM for DXM.
Tat72
Both significantly reduced TNF-α secretion. ED50 of 200 μm for MK-801 and 100 μM for DXM.
In vivo
DA levels
48 h after drug treatment, DA is just 20% of control in the striatum.
Mice receiving MK-801 before methamphetamine exposure showed a 55% reduction in DA depletion.
DXM also led to a reduction, resulting in DA depletion at 55% of control.
Neither DXM nor MK-801 alone led to striatal DA changes.
The neurotoxic regimen of methamphetameine also produced a substantial increase in microglial staining, which was significantly attenuated by MK-801 and DXM.
Temperature
Methamphetamine produced mild hyperthermia.
MK-801 preadministration led to body temperature being at control levels for the first 2 h then falling to 1-2°C below control for the last 6 h.
While with DXM, there was a fall of about 4°C and that hypothermia persisted for 4 h, but after that point mice developed a mild hyperthermia very similar to mice given only methamphetamine.
Neither DXM nor MK-801 altered body temperature alone.
COI: This research was supported by National Institutes of Health Grants DA10756 and DA014692, a VA Merit Award, and by the Pilot Project Program of the EHS Center in Molecular and Cellular Toxicology with Human Applications
(Li, 2005) – Protective against endotoxic shock in mice
Investigating its ability to protect against endotoxin shock induced by a combo of lipopolysaccharide/D-galactosamine (LPS/GaIN) in mice.
Main protocol: DXM (12.5 mg/kg SC) 30 min before and 2 and 4 hours after an injection of LPS/GaIN (20 μg/700 mg/kg IP).
Secondary protocol: DXM (12.5 mg/kg SC) given 30 min before or 30, 60, and 120 min after LPS/GaIN.
Results
Main protocol
DXM was found to significantly decrease LPS/GaIN-induced mortality and hepatotoxicity, as shown by higher survival rate, decreased AST activity, and improved pathology.
Survival
LPS/GaIN only – 45.9% survival
6.25 mg/kg DXM – 66.6% survival
12.5 mg/kg DXM – 89.3% survival
25 mg/kg DXM – 91.6% survival
Hepatotoxicity
While LPS/GaIN alone led to broad hemorrhagic necrosis and severe hepatocyte swelling and degeneration, DXM-treated animals rarely showed hepatic congestion and hepatic necrosis.
LPS/GaIN animals had a 35-fold rise in serum ALT, but this was significantly attenuated with DXM 30 min pre and post-treatment.
Protection likely came from a reduction in serum and liver TNF-α levels. Though, DXM also attenuated production of superoxide and intracellular ROS in Kupffer cells and neutrophils.
Endotoxin normally activates Kupffer cells to release inflammatory mediators like free radicals and ROS. The evidence indicates DXM inhibits TNF-α through a PHOX-ROS pathway.
Real-time PCR showed DXM suppressed the expression of a variety of inflammatory genes, including macrophage inflammatory protein-2, CXC chemokine, thrombospondin-1, intracellular adhesion molecular-1, and IL-6.
And it also attenuated the expression of cell-death related genes like GADD45 and GADD153.
Overall, it appears DXM is protective in mice against LPS/GaIN-induced hepatotoxicity. The protection appears to come from faster TNF-α clearance and lower superoxide production and inflammation and cell-death related components.
COI: Not reported
(Zhang, 2004) – DXM is neuroprotective in a Parkinson’s model in a partly NADPH oxidase-dependent manner
Mice. They were given daily SC injections of saline or MPTP (15 mg/kg) for 6 consecutive days.
DXM was given twice daily at 10 mg/kg for the first 6 days and then once-daily for the rest of the study.
Mice were killed either 6 or 21 days after their last MPTP injection.
Results
DXM protects neurons in the substantia nigra pars compacta (SNpc)
6 days later the mice were killed. Compared with saline mice, MPTP induced a significant decrease in tryptophan hydroxylase immunoreactivity in both the neuronal cell bodies and neuronal fibers.
There was a 30% loss of reactivity in the MPTP mice. Administration of DXM significantly reduced the loss of reactivity.
DXM inhibits MPTP-induced production of ROS in neuron-glia cultures
Mouse mesencephalic neuron-glia cultures were pretreated with DXM 1 μM for 30 min before MPTP 1 μM was added. DXM was then given 2 and 4 days after MPTP treatment. And on Day 6, release of superoxide from activated microglia was determined.
Treatment of cultures with DXM almsot fully inhibited the MPTP-induced superoxide production. DXM treatment significantly reduced the level of intracellular ROS from MPTP.
The role of NADPH oxidase
NADPH oxidase is the primary enzyme for the production of ROS, especially superoxide. It was hypothesized to play a role in the neuroprotection of DXM.
Mice lacking NADPH oxidase only showed a 14% loss of nigral TH-ir neurons after MPTP, compared with the 32% loss in regular mice.
This shows that in mice subchronically receiving MPTP, NADPH oxidase at least partially mediated the MPTP-induced loss of SNpc TH-ir neurons.
Role of NADPH oxidase in the effect of DXM
DXM was totally ineffective in protecting neurons in mice lacking the enzyme. This demonstrates that the neuroprotection is at least partly dependent on normal function of NADPH oxidase.
Catecholamine levels
MPTP induced similar degrees of depletion in the content of DA and DOPAC in mice with and without NADPH oxidase. Administration of DXM did not affect either the basal or MPTP-induced catecholamine level changes.
Nitrite production
Mouse mesencephalic neuron-glia cultures were pretreated with DXM 1 μM 30 minutes before MPTP 1 μM.
The levels of nitrite in cultures receiving both were significantly lower than in those only receiving MPTP, showing DXM at least partially suppresses MPTP-induced nitrite production.
COI: This work is supported in part by the New Investigator Award (to B.L.) from the College of Pharmacy of the University of Florida.
(Jimenez, 1999) – DXM at a low, but not high dose can improve levodopa-induced motor response in a model of Parkinsonism
Background
Preclinical studies have shown NMDA antagonists may potentiate the antiparkinsonian effect of levodopa while having little efficacy of their own in the condition.
Rats were given 6-OHDA lesions.
Experiment 1
They were treated for 22 days twice daily with levodopa at 25 mg/kg IP along with 6.25 mg/kg benserazide
Day 23: Received DXM 20, 30, or 40 mg/kg IP immediately before levodopa.
Experiment 2
Lesioned rats were treated with levodopa plus DXM for 22 consecutive days to see if chronic coadministration of DXM would prevent the decline in the duration of motor response from levodopa.
Results
Acute DXM
By Day 22 the response to levodopa declined significantly. Co-administration of DXM on Day 23 reduced the reduction in the duration of the levodopa response at the lowest dose of 20 mg/kg, but failed to work at at higher doses.
Chronic DXM
Chronic DXM did not provide much of an effect at any dose
COI: This study was supported by an award from ASTA MEDICA-PARKINSON ESPAN˜A, and grants from CIRIT 96-SGR00064 and SAF 97-0109 from Comisio´n Interministerial de Ciencia y Tecnolog´ıa
(Britton, 1997) – DXM protects against cerebral injury after transient, but not permanent, focal ischemia in rats
DXM’s impact was evaluated after transient (2 hour) and permanent focal cerebral ischemia in rats.
Given DXM at 20 mg/kg SC at 0.5, 1, 2, 4, and 6 hours post-occlusion.
DXM produced a 61% reduction in infarct volume from acute ischemia, but it did not significantly change the infarct volume post-permanent occlusion.
After transient ischemia, rectal temperature was elevated at 1, 2, and 5 hours post-occlusion. DXM attenuated this rise in temperature without inducing hypothermia and this action seemed to correlate with its protection of neurons in temperature-regulating hypothalamic centers.
COI: Not reported
(Duhaime, 1996) – DXM offers some neuroprotection in rats exposed to acute experimental subdural hematoma
68 rats were studied. They were spread across Series 1, Series 2, and Series 3.
Series 1
Experimental subdural hematoma induced using the “cranial window” modification. 14 animals received 10 mg/kg of long-acting DXM (Delsym) twice daily by nasogastric tube for 72 hours, with the first dose given at the time of subdural hematoma placement. Control animals received sterile water.
Animals were sacrificed at 72 hours.
Series 2
The same technique was used, though the anesthetic oxygen concentration was reduced to 21% in order to better replicate clinical conditions. Also, an initial IP dose of 20 mg/kg DXM was given to experimental animals at 15 minutes after placement of the clot. Then the animals received 10 mg/kg twice daily with the first dose beginning 72 hours after surgery.
Series 3
The same technique was used by the group had a narrower weight and age range.
Results
There was no significant difference in lesion volume between animals in the three groups. Animals given DXM, either oral alone or oral plus IP, had significantly smaller lesions than animals given placebo. There was no significant interaction between series and drug effect.
Neuroprotection by DXM does not appear to come from changes in brain temperature.
COI: Not reported
(Henderson, 1992) – DXM blocks the acute depletion of serotonin from ρ-chloroamphetamine, though likely just by binding to SERT.
Rats were given ρ-chloroamphetamine (PCA) 10 mg/kg IP 2 hours before being killed or they were given H75/12 40 mg/kg IP instead, which produces acute but not neurotoxic serotonin depletion
They received DXM 25 or 75 mg/kg IP 140 minutes before being killed.
Results
PCA caused a 47% depletion of serotonin in whole brain 2 hours after injection. It was totally prevented by 75 mg/kg DXM, but the 25 mg/kg dose was ineffective.
H75/12 also caused a 56% depletion of serotonin, which was antagonized significantly by both DXM doses.
DXM also decreased whole brain concentrations of 5-HIAA, which was significant at both doses. But it did not deplete serotonin.
Discussion
DXM is protective against PCA declines in serotonin and 5-HIAA, likely attributable to serotonin uptake blockage.
The DXM-induced decline in 5-HIAA is probably from blocking serotonin uptake and therefore metabolism.
COI: Study was completed by Eli Lilly and Company.
(Finnegan, 1991) – DXM is protective against the neurotoxic effects of PCA in rats
Groups
PCA 5 mg/kg alone
DXM 75 mg/kg alone
Combination of PCA and DXM (10 – 75 mg/kg)
DXM was given to the rats 20 min before PCA and the rats were killed 10 days later.
Results
PCA alone reduced serotonin concentration in the striatum, hippocampus, and cortex by 70-80%. PCA also induced depletions of 5-HIAA equivalent to the serotonin depletion in all brain areas.
DXM offered a dose-dependent protection against these declines. The 75 mg/kg dose provided nearly complete (84%) protection in the striatum, while it was 70% in the hippocampus and 74% in the cortex.
DXM administered alone had no significant impact on serotonin or 5-HIAA levels.
COI: Supported by a grant from the California Parkinson’s Foundation and the American Medical Association.
(Tortella, 1989) – DXM in rats can protect against post-ischemic hypoperfusion after transient global ischemia
Rats
Groups:
Saline before occlusion
DXM 20 mg/kg bolus 30 min before occlusion and initiation of 10 mg/kg/h at the onset of occlusion
DXM post-treatment at 2 mg/kg bolus followed by 10 mg/kg/h at the onset of post-ischemic hypoperfusion.
Sham-operated unoccluded controls otherwise treated like Group 2
3 hours after reperfusion the animals were killed.
Results
In the sham-operated rats, DXM bolus led to immediate hypotension and bradycardia
Group 1 – 15 min of cerebral ischemia produced a 90-95% decrease in CBF and an isoelectric EEG. Upon reperfusion there was an initial hyperemic response followed by a prolonged period of post-ischemic hypoperfusifon where CBF remained reduced through the whole observation period.
In DXM rats, significant improvements in CBF and EEG were seen. Pre-treatment delayed the onset of hyperemia and significantly reduced the latency to maximum hypoperfusion. Moreover, the max decrease in CBF was reduced to only 68% that of control and returned to baseline within 1-2 hours of reperfusion.
After 3 hour of reperfusion, CBF was significantly enhanced to 119% compared to Group 1 and EEG had returned to the pre-ischemic state.
Administration after the insult was also effective in normalizing CBF and EEG
COI: Research was conducted in compliance with the Animal Welfare Act, and other Federal statutes and regulations relating to animals and experiments involving animals and adheres to the principles stated in the Guide for the Care and Use of Laboratory Animals, NIH publications 85-23. The views of the authors do not purport to reflect the position of the Department of the Army or the Department of Defense, (para 4-3), AR 360-5.
(Steinberg, 1988) DXM and DXO can both reduce cerebral damage after ischemia in rabbits.
15 male rabbits. They underwent 1 h transient transorbital occlusion of the left internal carotid artery and distal A1 segment of the anterior cerebral artery.
One hour after procedure they received one of these IV:
DXM – 20 mg/kg loading dose followed by 10 mg/kg/h
DXO – 15 mg/kg loading dose followed by 15 mg/kg/h
Saline
The animals were killed 4 hours after reperfusion.
Results
Both drugs significantly decreased the neocortical area of severe ischemic neuronal damage (SIND). The DXM rabbits had a 3.7% SIND, the DXO rabbits a 4.4%, and the saline group had a 41.3% rate. There was no significant difference between drugs for degree of cerebral protection.
COI: Supported in part by an NIH Biochemical Research Support grant.
(George, 1988) – Reduces neocortical damage from ischemia.
Rabbits. Randomly assigned to either 20 mg/kg IV bolus followed by 10 mg/kg/h of dextromethorphan or saline.
They were exposed to a 1 hour occlusion of the left internal carotid artery and anterior cerebral artery followed by 4 hours of reperfusion.
DXM animals showed a significant decline in the % of severe neocortical ischemic neuronal damage (10.5% vs. 49.6%).
In the striatum, there was also a trend towards less damage with DXM, but it didn’t reach significance. Only in the most posterior putamen did the protective effect of DXM on severe ischemic neuronal damage become significant.
COI: Not reported
Ineffective
(Engber, 1988) – DXM failed to protect against quinolinic acid neurotoxicity in rat striatum
DXM (40 or 80 mg/kg IP) was tested, as was MK-801 (3 or 10 mg/kg IP). Measuring the impact of quinolinic acid (300 or 150 nM injection into the striatum) on depletion of choline acetyltransferase (ChAT) activity.
While MK-801 at 3 mg/kg was able to significantly reduce depletion of ChAT and fully blocked depletion at 10 mg/kg, DXM failed to protect striatal cholinergic neurons.
Behavioral
Both drugs impacted motor behavior. DXM 40 mg/kg led to moderate ataxia, similar to MK-801 3 mg/kg. But that same dose of MK-801 also led to stereotyped lateral head movements, which were not seen in DXM. And while 80 mg/kg of DXM produced severe ataxia and occasional lateral head movements, MK-801 at 10 mg/kg always produced those head movements.
COI: Not reported
In vitro/Ex vivo
Effective
(Cheng, 2015) – DXM is neuroprotective in vitro in mouse BV2 microglia in a LPS-stimulation test
BV2 mouse microglial cells were studied. DXM was used at 10 μM
The levels of the p65 subunit of NFκB were significantly increased after LPS vs. control. But those levels were significantly attenuated by DXM. Subsequent to LPS, caspase-3 expression was also significantly suppressed after DXM vs. after just LPS.
DXM inhibited a rise in HSP60 expression and release from activated BV2 cells. HSF-1 expression levels were also significantly upregulated by LPS and significantly downregulated by DXM.
DXM may be considered to effectively inhibit HSP60, HSF-1, NKκB, caspase-3, and iNOS expression in LPS-stimulated microglia.
COI: This study was supported by the National Natural Science Foundation of China (grant nos. 31060140 and 31260243), the Project‑sponsored by SRF for ROCS and State Education Ministry. Additional funding was provided to Dr Yin Wang by the Program for New Century Excellent Talents in University.
(Lisak, 2014) – DXM protects glial cells from cytotoxic molecules
In vitro study of its impact on oligodendroglial cells and oligodendroglial progenitors. Enriched gligal cultures from newborn rats were used.
Cytotoxicity studies: DXM tested at different concentrations for 1-3 days to determine if it was toxic. Based on those results, it was then assessed if DXM could protect OL/OPC. A range of concentrations, focusing on 1-2 μM, was used. Those doses have been shown to protect CNS in rats treated with DXM/quinidine.
DXM was preapplied for 30 min and then various toxic agents were applied. Cultures examined after 24 hours to see the impact.
Results
DXM began to cause cell death with higher levels, while minimally causing it at 1-2 μM.
DXM had a significant effect on glial proliferation in less mature cells, with small variable effects in mature cultures. 1 μM DXM was able to stimulate proliferation of oligodendroglial progenitors (OPC) by 4-fold, microglia by 2.5-fold, and astroglia by 2-fold.
Treatment of OPC with DXM for 3 days was able to increase the % of OPC relative to oligodendroglial, with a smaller difference by Day 5, indicating maturation of OPC to OL was increasing.
DXM at 2 and 20 μM protected both OPC and OL from death via glutamate, NMDA, AMPA, quinolinic acid, staurosporine, and ROS exposure.
COI: Grant sponsors included Avanir Pharmaceuticals, the Parker Webber Endowed Chair in Neurology, and a National Multiple Sclerosis Society Collaborative Research Center Award.
(Li, 2005) – Femtomolar concentrations can protect mesencephalic neurons from inflammatory damage
Mice and rats were used to obtain neuronal or neuron-glia cultures. Cultures were pretreated with DXM 30 min before exposure to LPS.
Results
DXM is neuroprotective across a wide range of concentrations, from 10-5 to 10-17.
Neuron-glia cultures were exposed to LPS and then seven days later the degeneration of dopaminergic neurons was studied based on DA uptake. DXM was able to attenuate across those concentrations the decline in DA uptake.
Nanomolar and picomolar concentrations, however, did not provide protection, indicating a bimodal response.
Treatment with LPS also led to a significant decline in TH-IR neurons. 30 min pretreatment with DXM 10-5 and 10-14 produced significant attenuation of that impact, while DXM at 10-10 did not work.
Glia are essential for femtomolar neuroprotection
Nine days after treatment with 4 μM of Aβ 1-42, DA uptake was reduced by 50% vs. control. Pretreatment with DXM across concentrations did not significantly alter this decline in DA uptake in the cultures, suggesting the presence of glia is necessary for DXM to exert neuroprotection.
Femtomolar concentrations were shown to inhibit LPS-induced microglia overactivation and the subsequent release of inflammatory factors. Pretreatment significantly decreased the release of NO, PGE2, TNF-α, though again DXM 10-10 did not work.
Pretreatment also significantly reduced the induced release of superoxide and intracellular ROS.
ROS are involved in the neuroprotection
Neuron-glia cultures from NADPH oxidase lacking mice had a 25% reduction in uptake capacity, while wild-type mice had a 46% reduction. DXM significantly attenuated the effect of LPS in the WT mice but not in those lacking NADPH oxidase.
Similar results were seen for iROS production, which is only half as great in NADPH oxidase negative mice and in those mice DXM is ineffective.
LPS-induced TNF-α production in WT mice is greater and reactive to DXM, while that is not the case in the NADPH oxidase lacking mice.
DXM was also found to be effective even when applied after the insult
LPS was given for 12 hours, then removed. DXM was then added to the cultures and incubation continued for another 6 or 7 days. The presence of LPS in the media for only 12 hours was able to reduce DA uptake capacity by 70%, while post-treatment with DXM at 10-5 and 10-14, but not 10-10, was effective.
COI: Not reported
(Zhang, 2004) – 3-HM, a metabolite of DXM, is protective and neurotrophic to dopaminergic neurons
This study used primary mesencephalic neuron-glia cultures, but focused on 3-hydroxymorphinan (3-HM), a metabolite of DXM.
3-HM is O- and N-demethylated DXM.
Results
3-HM is neurotrophic to dopaminergic neurons and is neuroprotective against LPS-induced dopaminergic neurotoxicity
3-HM (5 μM) can reverse LPS-induced declines in DA uptake nearly back to control values. And treatment with 1-5 μM of 3-HM alone can itself increase DA uptake capacity by 20-60% vs. control, indicating a neurotrophic effect.
Pretreatment with 3-HM (5 μM) significantly restored LPS-induced reduction in the number of dopaminergic neurons to 97% of the control value. It also improves morphological signs of dopaminergic neuron health.
The neurotrophic effect of 3-HM is glia-dependent
Unlike DXM, 3-HM produces a significant neurotrophic effect in mesencephalic neuron-glia cultures. That effect disappears when using neuron-enrinched cultures, indicating the neurotrophic action isn’t from a direct effect on dopaminergic neurons, but rather is glia-dependent.
Astroglia appear responsible for the neurotrophic effect of 3-HM.
Lower doses of 3-HM , such as 0.3 μM, can protect dopaminergic neurons but lack the same neurotrophic effect.
Microglia mediate the 3-HM-induced neuroprotective effect. Adding 3-HM to cultures before exposing them to LPS can attenuate LPS-induced microglia activation along with preventing the loss of dopaminergic neurons.
3-HM can attenuate the LPS-induced increase in ROS, including extracellular superoxide and iROS. It also reduces the rise in TNF-α and the release of nitrite (an indicator of LPS-induced nitric oxide production), along with the rise in PGE2.
COI: Not reported
(Liu, 2003) – DXM protects dopaminergic neurons from inflammation-mediated degeneration. This effect is microglia-dependent
Primary mesencephalic neuron-glia cultures were prepared from the brains of rats.
Results
DXM protects against LPS-induced degeneration of dopaminergic neurons
Mesencephalic neuron-glia cultures were pretreated with vehicle or 1-10 μM DXM for 30 min before exposure to LPS. Seven days later, the degeneration of neurons was assessed.
DA uptake results show LPS treatment reduced uptake capacity to 37% of control and DXM significantly attenuated this change in a dose-dependent manner.
Counting the number of TH-ir neurons, there was a reduction of 71% with LPS, but DXM at 10 μM significantly protected against this.
Morphologically, the dendrites of TH-ir neurons were significantly less elaborate after LPS, but they were protected significantly by DXM. The average dendrite length in LPS cultures was just 5.2% that of control cultures, whereas it was 81% of control with DXM 10 μM.
Significant neuroprotection was possible up to 60 min after LPS exposure, but not if given 120 or 180 min after exposure.
DXM is not protective against degeneration caused by MPP+ or Aβ
5 days after treatment with 2 μM MPP+ or 8 μM Aβ, the cultures were compared to control. Pretreatment with DXM 10 μM failed to significantly alter the magnitude of reduction of DA uptake.
DXM dose-dependently inhibited the stimulation of superoxide production by LPS. Significant inhibition was seen starting at 2.5 μM and there was near complete inhibition of superoxide production at 10 μM.
Superoxide increases were not prevented in a model looking for superoxide scavenging properties, indicating the reduction of superoxide is not due to scavenging by DXM.
COI: Not reported
(Choi, 1987) – DXM and DXO protect against glutamate neurotoxicity in vitro
In vitro study using mixed cortical cell cultures including neuronal and glial elements. Cultures from mice.
Neuronal injury was assessed based on the extracellular level of the cytosolic enzyme lactate dehydrogenase (LDH) and based on morphology. LDH was measured 2 days after glutamate exposure.
Results
Exposure to 0.5 mM of glutamate for 5 min produced disintegration of the majority of neurons.
If 100 μM DXO was added before exposure, the morphological and LDH evidence showed marked attenuation of damage.
10 μM reduced the protective effect somewhat, while 1 μM was barely effective.
Exposure just to 100 μM DXO did not produce evidence of neuronal damage.
With 100 μM DXM, a similar protective effect was seen, based on LDH and morphological evidence.
COI: Supported by grants from the Wills Foundation and the Hereditary Disease Foundation.
Depression
There is limited human evidence supporting DXM for depression, but it has received some attention in part because of the rise of ketamine as a fast-acting antidepressant. DXM and ketamine share some of their pharmacology and since DXM has a more substantial history of use, it could be a good antidepressant if efficacy is shown.
In humans, a combo of DXM and quinidine significantly reduced depression over a 10-week period, with a response rate of 45% and a remission rate of 35% (Murrough, 2017). Those effects were seen in people with a median of 2.5 failed antidepressant trials in the past.
Animal studies find it has antidepressant-like properties in the tail suspension test (TST) and forced swim test (FST) (Nguyen, 2016), two very common stress tests that are meant to find potential antidepressants. Blocking σ1 or AMPAR can attenuate the benefits (Nguyen, 2015 ; Nguyen, 2014). DXM hypothetically indirectly activates AMPAR, which could raise BDNF levels (a proposed route towards antidepressant effects). AMPAR seems to be involved in the efficacy of both DXM and ketamine.
Though the literature typically supports the antidepressant properties of acute DXM administration, subchronic administration at sufficiently high doses could have a negative effect. According to Po (2015), 40 mg/kg IP for two weeks produced depression-like symptoms and significantly impaired the proliferation of new cells in the dentate gyrus, lowered the number of immature neurons, and suppressed the growth of immature neurons. Because these results contradict other studies, DXM’s ability to promote or inhibit neurogenesis could be dose-related.
DXM does bind to multiple sites, such as σ1, SERT, and NMDAR that have been implicated in the effects of other antidepressants. Many antidepressants bind to σ1, for example, and σ1 knockout mice show depression-like symptoms, suggesting agonism (like with DXM) could be useful. And there is an interaction between σ1 and serotonin, with sigma agonists raising serotonergic activity in the dorsal raphe faster than conventional antidepressants. Ketamine’s fast-acting potentiation of nerve growth factor (NGF)-induced neurite outgrowth may also be σ1 dependent.
Human
Effective
(Murrough, 2017) – Combo of DXM and quinidine is effective for treatment-resistant depression.
Phase 2 open label clinical trial combining DXM with quinidine.
20 patients. They received up to 45 mg DXM and 10 mg quinidine every 12 hours over the course of a 10-week period.
They had a history of failure to respond to a median of 2.5 lifetime adequate antidepressant trials.
Results
14/20 completed. Of those who didn’t, 3 discontinued due to poor tolerability of the drug, 1 discontinued for unspecified reasons, 1 was withdrawn due to psychiatric hospitalization, and 1 was withdrawn due to non-adherence.
No treatment-emergent suicidal ideation, psychotomimetic, or dissociative symptoms were seen.
MADRS score dropped by -13 (p<0.001). And QIDS-SR score dropped a mean of 5.9 points (p<0.01)
Response rate of 45% and remission rate of 35% based on the ITT sample (all 20 patients.)
50% of patients were rated improved or very much improved.
COI: Not reported
Ineffective
(Lauterbach, 2016) – A case report in which DXM appeared to have fast-acting and subacute antidepressant effects, but in which daily dosing did not remain effective.
51-year-old male with recurrent, severe, nonpsychotic depression, along with anxiety. He went through multiple medication trials, including bupropion, vortioxetine, fluoxetine, and paroxetine. Most medications helped for a period of months before becoming ineffective.
During a trial of bupropion, the drug was ineffective after 2 weeks of bupropion XL 600 mg.
DXM was initiated during that trial:
300 mg oral (Delsym) was added. After his first dose, he reported euthymia with full depression resolution, somewhere between 3 and 6 hours post-dose.
After the second 300 mg oral dose on the same day he had adverse effects like nausea, dizziness, blurred vision, and lethargy.
DXM was then reduced to 30 mg oral twice daily and this was continued from Day 2 to Day 9, at which time he felt he may be relapsing and dose was increased to 60 mg twice daily on Day 10. On Day 12 he had full remission of all symptoms within 48 hours of starting that dose.
He continued to do well with that dosage for 20 days, but on Day 32 he had an onset of labile intraday variability in fatigue and irritability that gradually worsened into full relapse by Day 39.
DXM was then discontinued, as was bupropion.
COI: Not reported
Animal
Effective
(Nguyen, 2017) – Deuterated DXM has antidepressant effects in mice, but they’re unaffected by blocking AMPA receptors, unlike with normal DXM.
Mice received IP injections of drugs 30 min before FST and TST. Pretreatment with NBQX, BD1063, or BD1047 occurred 15 min prior to DXM.
Results
Effects of deuterated DXM on the FST, TST, and open field test
It significantly decreased immobility time in the FST and TST, similar to the positive control imipramine. At 30 mg/kg it was significantly different from saline. And in the OFT, it significantly increased locomotor activity, whereas imipramine reduced locomotion.
No correlation between reduction in immobility time and increase in locomotion, meaning that does not account for the antidepressant-like effects.
Effect of AMPA or σ1 antagonists on DXM
Pretreatment with the AMPA antagonist NBQX at 30 mg/kg failed to prevent the antidepressant-like effects of deuterated DXM in the FST.
Pretreatment with the σ1 antagonist BD1063 at 10 mg/kg or BD1047 at 20 mg/kg had a trend towards attenuation of the antidepressant effects.
The overall ANOVA was significant for the pretreatment studies. BD1063+DXM still significantly differed from saline, while BD1047+DXM did not. This indicates partial attenuation of the effects.
Effect of quinidine
Quinidine 30 mg/kg failed to significantly influence the antidepressant effects. The highest dose of DXM, 30 mg/kg, did not produce a significant effect when combined with quinidine vs. saline. And in locomotor tests, quinidine significantly reduced the stimulatory action of DXM.
COI: R.R.M. received research funding from Avanir Pharmaceuticals, Inc.
(Nguyen, 2016) – DXM reduces immobility time similarly to the fast-acting antidepressant ketamine
Mice
Results
Both ketamine and imipramine reduced immobility time in the FST. DXM similarly reduced immobility time.
Ketamine significantly increased locomotor activity, while imipramine and DXM did not.
BDNF
Pro-BDNF was significantly increased by ketamine in the hippocampus but not the frontal cortex 40 min after injection. Imipramine did not alter pro-BDNF in either region, nor did DXM.
For the mature form of BDNF, no alterations in protein expression were seen in either region for any drug tested.
COI: None
(Nguyen, 2015) – AMPA receptors, at least indirectly, play a role in the antidepressant effects of DXM.
Mice were used and given both DXM and quinidine.
Results
Effects of imipramine, ketamine, and DXM in the TST.
All drugs significantly reduced immobility time and 30 mg/kg (IP) DXM was significantly different from placebo.
CYP2D6 inhibition potentiates DXM’s effect in the TST
Concurrent administration of 30 mg/kg (IP) quinidine can potentiate the antidepressant-like effects of DXM 10 mg/kg, which is otherwise not significantly different from placebo.
NBQX, an AMPA antagonist, attenuates the antidepressant-like effects
Pretreatment with NBQX 10 or 30 mg/kg (IP), which is behaviorally inactive on its own, attenuates the antidepressant-like effect of DXM, ketamine, and imipramine in the TST.
AMPA antagonism can also attenuate the effects of DXM and ketamine, but not imipramine, in the FST
COI: Author has received funding from Avanir Pharmaceuticals.
(Nguyen, 2014) – Sigma 1 receptors are involved in antidepressant activity from DXM
Mice were given the experimental drugs via IP.
Results
DXM dose-response
DXM significantly reduced immobility time at 30 mg/kg. It also generally increased locomotor activity, but a correlation between the DXM-induced rise in locomotor activity and decrease in immobility time was not seen.
σ1 antagonists dose-response
The σ1 antagonist BD1063 itself significantly reduced immobility time at 30 mg/kg, but not at 10 mg/kg, so that dose was used in the antagonist testing.
BD1047 had no significant effect on the forced swim test at any dose.
Impact of σ1 antagonism on DXM or imipramine
Behaviorally inactive doses of BD1063 or BD1047 attenuated the antidepressant-like effects of DXM, but not imipramine. This was only trend-level for BD1047.
BD1063’s impact on DXM dose-response
With a single 10 mg/kg dose of BD1063 against different doses of DXM, its presence shifted the dose-response curve for DXM to the right.
Effect of CYP2D6 inhibition
Quinidine (30 mg/kg) along with DXM potentiated the antidepressant effect, implicating DXM itself in the efficacy, not its DXO metabolite.
Importantly, DXM 10 mg/kg was not significantly different from saline, but with quinidine it significantly decreased immobility time.
In locomotor tests, DXM with quinidine elicited no stimulant effect.
Fluoxetine, just like in other studies, didn’t have acute antidepressant-like effects in this animal test.
Further σ1 binding tests support the presence of at least two distinct sites or modes of interaction with which DXM binds to the σ1 receptor. One has competitive interactions and the other has non-competitive interactions.
COI: Not reported
Ineffective
(Po, 2015) – Subchronic DXM decreases neurogenesis and results in depression-like behavior in rats
Rats. They were placed into groups:
Control
DXM 40 mg/kg per day IP for 14 days
Behavioral testing was completed on Day 15. Four hours later, the animals were killed to obtain tissue samples for immunohistochemistry.
Results
DXM significantly increased immobility time in both the FST and TST compared to control group.
It significantly decreased the number of positive social interactions when compared to control.
And the duration of time in the center area of the open field test was significantly lower vs. control.
Neurogenesis
DXM significantly decreased the proliferation of new cells in the dentate gyrus vs. control. But it had no impact on the survival of new cells in the dentate gyrus (DG).
DXM significantly decreased the number of immature neurons based on DCX-immunoreactivity.
Co-immunostaining with BrdU and DCX shows that DXM brought a reduction in proportion of BrdU-immunoreactive cells with DCX expression, indicating it suppresses neuronal differentiation of new cells in the DG.
DXM animals also showed significantly less complex dendritic structure vs. control, indicating it suppresses the growth of immature neurons.
COI: The current study is supported by the departmental general research grant, Department of Rehabilitation Science, The Hong Kong Polytechnic University.
Parkinson’s Disease
DXM is not very effective in Parkinson’s disease, based on the current evidence. Two pilot studies with 90 and 180 mg/d failed to show any benefit (Montastruc, 1994). Another study did show some beneficial effects (largely on levodopa-induced dyskinesias) in 6 out of 18 patients with 60-120 mg/d, but the effect sizes were small and the p values weren’t very significant (Metman, 1998).
One of the main areas of investigation was in reducing levodopa-induced dyskinesias, which occur in a most Parkinson’s patients after years of treatment. Those motor issues may involve chronic atypical dopaminergic stimulation activating signalling pathways that potentiate the synaptic efficacy of NMDARs expressed on striatal neurons. Blocking NMDARs in animals can reverse or prevent motor issues from chronic levodopa.
Effective
(Metman, 1998) and (Metman, 1998) – DXM might improve symptoms in a small portion of people
18 patients with Parkinson’s disease were included. 6/18 reported a beneficial effect at their individually determined optimal dose of 60-120 mg/d.
The 12 remaining patients had reversible side effects (particularly mild drowsiness) or decreased levodopa efficacy, and were then excluded from the study.
Of the 6 responders, they were placed in a double-blind placebo-controlled crossover study with two 2-week arms and a washout.
Measures were taken on the last day of each arm. Motor ratings were performed every 20 min for 8 consecutive arms.
They received DXM twice daily for 2-3 weeks in a double-blind, crossover style with placebo. The dose gradually increased to reach 180 mg/d or a max tolerated dose. Quinidine (100 mg twice daily) was also given orally throughout the study to normalize the kinetic parameters of DXM.
Results
DXM reduced the dyskinetic effect of levodopa. At each patient’s highest levodopa dose, the average and max dyskinesia scores were lower during the DXM arm, though only 59% vs. 54% (p=0.03).
Parkinsonian scores were lower with DXM than with placebo, though only p=0.04.
Pharmacokinetics
DXM levels measured 8 hours after the morning dose were only slightly lower than 2 hours after. DXM levels were around 3 times higher than DXO levels, indicating adequate CYP2D6 inhibition.
Adverse
3 subjects had no side effects. The other 3 complained of feeling “drugged” at 120 mg (2 patients) and 90 mg (1), but those symptoms went away during the treatment period.
COI: Supported by the Parkinson Foundation of Canada, the Parkinson Patients Foundation of the Netherlands, and by the National Parkinson Foundation.
Ineffective
(Montastruc, 1994) – Two pilot studies failing to show benefit in Parkinson’s Disease patients
Study 1
30 mg three times per day in 13 nondemented Parkinson’s Disease patients
10/13 completed the study
The dropouts were attributed to major sedation with urinary incontinence; pruritus with nausea after the first dose; feeling of sickness after 2 weeks.
Results
Add-on therapy with DXM 90 mg/d failed to modify parkinsonian symptoms. And the UPDRS subscores for cardinal extrapyramidal symptoms (tremor, rigidity, bradykinesia), mentation, behavior and mood, or for daily activities also didn’t change.
Study 2
60 mg three times per day in 8 nondemented Parkinson’s Disease patients
4/8 completed the study
Dropouts for major sedation; dizziness; and severe cutaneous dysesthesia
Results
Add-on therapy with DXM 180 mg/d failed to modify global or partial UPDRA scores.
COI: Not reported
Alzheimer’s Disease
Psychiatric symptoms are common in Alzheimer’s, with agitation being one of the most common. Few treatments for agitation exist other than atypical antipsychotics, with may come with modest efficacy and frequently have a notable side effect burden. DXM is therefore of interest due to some evidence indicating it can significantly control agitation and aggression (Ballard, 2015).
A large controlled trial of 220 patients found 30 mg DXM (with quinidine) significantly reduced agitation and aggression (p<0.01) while coming with minimal serious side effects and no cognitive impairment or sedation (Cummings, 2015).
In response to the Cummings et al. trial, Jacqui Wise in the British Medical Journal commented: “Pending further evidence, there is a reasonable strong case to prioritize dextromethorphan quinidine as an off-label treatment for agitation, possibly as a safer alternative to atypical antipsychotics.” (Wise, 2015)
And Dr. Karl Steinberg said the combination looks promising and is already being used off label for dementia-related agitation (Zoler, 2015):
Many clinicians have been using this product off-label for dementia-related agitation, although coverage can be a challenge and it is priced very high (over $700 a month) for those paying cash for it. It will be a welcome addition to the armamentarium if and when it is FDA approved for this indication, and certainly appears to be much safer than currently available off-label alternatives like antipsychotics. Although in my experience it’s not dramatically effective, dextromethorphan/quinidine has definitely provided appreciable improvement in some of my agitated nursing home residents with dementias —probably more noticeably in those with vascular dementia and emotional lability, although that’s not the indication being studied for possible FDA approval.
(Cummings, 2015) – DXM significantly improves agitation in patients with Alzheimer’s
220 patients were randomized to DXM or placebo. And in a second stage, those who had received placebo were rerandomized to expose a portion to DXM.
Dose eventually reached 30 mg DXM and 10 mg quinidine twice daily.
Total of 194 (88.2%) completed the study.
DXM significantly reduced agitation/aggression scores vs. placebo (P<0.01) in both Stage 1 and Stage 2 of the study.
Adverse
Serious adverse events occurred in 7.9% of DXM/quinidine patients vs. 4.7% with placebo.
Falls (8.6% with DXM vs 3.9% with placebo), diarrhea (5.9% vs. 3.1%), and urinary tract infection (5.3% vs. 3.9%).
It was not associated with cognitive impairment, sedation, or clinically significant QTc prolongation.
COI: Funded by Avanir Pharmaceuticals. Avanir had a role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; and preparation, review, or approval of the manuscript; the sponsor had no veto rights regarding the decision to submit the manuscript for publication.
Authors have been consultants for pharmaceutical companies, including Avanir Pharmaceuticals. They’ve received research support from pharmaceutical companies.
ALS
DXM does not appear effective in ALS. A study with 1.5 mg/kg per day in 49 patients failed to show any benefit and it also wasn’t effective in a trial of 14 patients (Blin, 1996 ; Askmark, 1993).
(Blin, 1996) – Not effective in ALS.
49 patients. Average duration of disease of 12.5 months.
Dose: 1.5 mg/kg per day for the whole trial
Results
At 12 months, there was no significant difference in the deterioration rate or the mortality rate between groups.
COI: Not reported
(Askmark, 1993) – Not effective
14 patients with ALS. They were given 150 mg DXM per day or placebo for 12-weeks in a double-blind trial, then an open trial of 300 mg/d was conducted for 3-6 months.
Results
No positive clinical or neurophysiological changes.
COI: The study was supported by the NHR Foundation, Sweden, and the Swedish Medical Research Council.
Huntington’s Disease
A single study of 11 patients showed no benefit, significant side effects, and clinical worsening (Walker, 1989). It was thought the drug could be helpful because of the motor effects of sigma receptor ligands and due to NMDAR antagonists possibly protecting against the excitotoxic cell death believed to play a role in Huntington’s.
(Walker, 1989) – Lack of benefit; worsening of symptoms and not tolerable
11 patients
Escalating doses of DXM for 4-8 weeks in most cases, from a starting dose of 120 mg/d increasing by 30-60 mg/d every 3 days.
Results
7/11 patients had significant side effects like eczematoid rash, clumsiness, dysarthria, drowsiness, or worsening of rigidity that led to limitations of dose increases or dose reduction.
Remaining 4 patients reached target doses of 120 mg (one), 480 mg (one), or 960 mg (two). 3 of those had minor symptoms.
Overall, patients had mild but significant clinical worsening on functional scores and quantitative exam scores vs. pre-drug and at maximal tolerated doses.
There were improvements in finger tapping and stepping, but since other scores declined, these “improvements” could have been the result of a training effect.
Many patients who didn’t report significant symptoms during dose escalation voiced definite improvements during DXM withdrawal. No exacerbations post-withdrawal were seen.
COI: Work supported by a grant from the Hereditary Disease Foundation.
Schizophrenia
DXM was beneficial as an add-on drug to risperidone therapy in two studies. One found a generally significant effect (Chen, 2012) while the other only showed a significant benefit of DXM on certain negative symptoms specifically in patients with the ALDH2*2/2 polymorphism (Lee, 2015). ALDH2 is an enzyme that affects the levels of dopamine metabolites.
A hypothetical mechanism of efficacy involves countering inflammation, which could mediate neurodegeneration and/or psychiatric problems in schizophrenia. DXM has neuroprotective properties, so it could hypothetically protect against the action of inflammatory cytokines crossing the blood-brain barrier. Higher levels of peripheral inflammatory markers have been found in schizophrenia patients.
(Lee, 2015) – DXM may improve negative symptoms in schizophrenia patients, specifically in those with a certain ALDH2 polymorphism.
Background
One of the genes involved in dopamine metabolism is ALDH2. It’s the major ALDH isozyme that catalyzes the oxidation of DOPAL to DOPAC.
Enzymes encoded by the ALDH2*1/2 or 2/2 polymorphism are partially or entirely inactive, respectively. Though the “2” allele is rarely seen in Caucasians it occurs in about 50% of the Asian population.
The ALDH2 gene is primarily associated with alcohol drinking behavior, but it may also be important in dopaminergic conditions due to its role on that neurotransmitter’s metabolism.
The ALDH2 deficiency caused by the ALDH2*2/2 genotype might cause DOPAL to accumulate, which could be toxic to dopamine neurons.
Schizophrenia patients were given either Risperidone+DXM 60 mg or Risperidone+Placebo for 11 weeks in a double-blind, randomized trial.
149 patients were recruited. 42 eventually dropped out, while 95 patients completed the study.
There were no significant differences in demographic, clinical, or genetic factors between those groups.
Results
PANSS and SANS scores were significantly lower by the end of treatment in both groups. DXM patients did not have significantly better outcomes.
Symptom attenuation associated with ALDH2 status
A significant association between improvement on the SANS total score and add-on DXM treatment was seen for the ALDH2*2/2 polymorphism. However, the ALDH2 polymorphism was not significantly associated with the PANSS total score or negative symptom subscale.
The interactive variable of DXM*treatment duration, reflecting the effect of add-on DXM on negative symptoms after the full treatment course, did show a significant change.
When examining the association between add-on DXM and changes in the 5 SANS subscales in patients with ALDH2*2/2 genotype, significant attenuation was found in the affective flattening, alogia, and attention subscales. Even after correcting for multiple comparisons, with the exception of the subscale for attention, the positive findings on SANS total and the other subscales remained.
COI: None. The work was supported by the Taiwan National Science Council, Taiwan Department of Health, the Taiwan National Health Research Institute, and the National Cheng Kung University Project for Promoting Academic Excellence and Developing World Class Research Centers.
(Chen, 2012) – Benefit of DXM in schizophrenia along with risperidone; connection between inflammatory markers and schizophrenia
100 healthy controls and 95 patients with schizophrenia tested in a double-blind manner.
Patients received either risperidone only (1-6 mg/d with a mean dose of 3-4 mg/d) or risperidone w/ dextromethorphan (DXM at 60 mg/d)
Results
Pretreatment, plasma levels of IL-1b and TNF-α were significantly greater in schizophrenic patients vs. controls. But plasma BDNF was significantly lower.
PANSS scores and plasma IL-1b levels significantly declined with treatment.
With the risperidone-only treatment, plasma TNF-a and BDNF increased significantly after 11 weeks.
But patients also receiving DXM showed a greater and earlier reduction in symptoms, along with an attenuated rise in the risperidone-induced increase in TNF-α.
COI: None
Methotrexate Toxicity
A few papers have demonstrated beneficial effects in methotrexate toxicity in a small number of patients (Afshar, 2014 ; Drachtman, 2002). Because methotrexate is a folate antagonist, it could disrupt the methylation of homocysteine, thereby leading to NMDA agonism and neurological symptoms. DXM’s inhibition of excitatory activity could be helpful.
DXM produced a complete resolution of symptoms like hemiparesis and dysarthria in 5 patients (Drachtman, 2002) and the majority of 18 patients improved after DXM treatment in another study (Afshar, 2014).
(Fernandez-Fernandez, 2017) – Recommends the use of DXM and methylxanthines for methotrexate-induced neurotoxicity
The authors are responding to a report about a 15-year-old male with delayed-onset methotrexate neurotoxicity.
They recommend that methylxanthines be used since a potential mechanism of the toxicity is the build up of adenosine in the CNS.
They also recommend DXM based on evidence showing it may be efficacious due to its ability to counter the excitotoxic effect of the homocysteine and its metabolities, which are agonists at NMDA receptors.
COI: None
(Afshar, 2014) – DXM appeared useful in the treatment of subacute methotrexate toxicity
The dose for these patients was 1-3 mg/kg per day. It was given after the sudden onset of neurological impairments post-methotrexate exposure.
Mean age: 11.2 years
Most patients had a diagnosis of acute lymphoblastic leukemia
Group A
8 patients started DXM over 24 hours after the start of their symptoms.
Average treatment response time was 13.9 hours.
Group B
10 patients started DXM an average of 7.6 hours after the start of their symptoms.
Most improved within 3.5 hours of receiving DXM.
Patient 1 had a seizure before DXM and also had slurred speech. After DXM, no more seizure activity was noted and slurred speech began to resolve within 12 min and fully resolved in 2 hours.
Patient 15 was given DXM 48 hours after his first seizure activity. Two more episodes were suffered, one 8 hours before DXM and one 12 hours after starting.
Patient 18 had been symptomatic for 10 days and then started to improve within 7 hr of receiving DXM.
16/18 patients fully recovered.
Discussion
DXM led to symptomatic improvement in most patients. Though placebo could be a factor and spontaneous resolution could have occurred in the patients without DXM.
COI: Not available
(Drachtman, 2002) – DXM is effective in the treatment of methotrexate neurotoxicity, according to results in 5 patients
5 patients with sudden onset of neurologic dysfunction while receiving methotrexate for malignant diseases were treated with DXM at 1-2 mg/kg/dose.
Results
The 5 patients had progressive neurological symptoms 1-2 weeks after a dose of methotrexate. They often had dysarthria, cranial nerve VII palsy, and hemiparesis. In all 5, DXM produced a complete resolution of neurologic deficits.
One patient had methotrexate neurotoxicity twice after the use of it for non-Hodgkin lymphoma.
The first time had was not treated for the toxicity and it went away gradually over 2 weeks.
The second time it developed, a month later, the patient received DXM and within 3 hours there was marked improvement, with complete resolution by the following day.
COI: Not reported
Epilepsy
It has anticonvulsant properties in animals in some settings (Wong, 1988 ; Tortella, 1986), but those properties have been minimally explored in humans (Wieser, 1992).
Humans
(Wieser, 1992) – Case report of reduced seizure duration and frequency. The epilepsy had been refractory.
48-year-old female with a 24-year history of medically refractory complex partial seizures and sometimes tonic-clonic seizures.
Seizures lasted for about 1 min and had a frequency of 2-28x per month.
Occasional tonic-clonic seizures with biting of the tongue occurred with a frequency of about 6 times per year.
Adequate control of tonic-clonic seizures was possible with tegretol, but the partial seizures were unresponsive to mesantoin, depakine, and rivotril.
MRI and CT showed no structural lesions. EEG revealed pronounced interictal spiking in the right mediabasal temporal lobe.
A right amygdalohippocampectomy was performed in 1987. Most probably due to spasms of the right anterior choroidal artery during surgery, postoperatively she had transient hemiparesis of the left side, which disappeared almost entirely by 2 months.
Postoperative scalp EEG showed no change in the right temporal interictal activity.
After a seizure-free period of 40 days she had complex partial seizures recurring with a frequency of 8.4 per month (average).
All attempted drugs (tegretol, mysoline, urbanyl, and oxcarbamazepine) were unsuccessful in controlling partial seizure frequency.
1991 – Patient herself began taking DXM 6-7 mg in the evening. She then reported seizure frequency declining significantly from 8.4 to 4.4 per month. Duration, according to witnesses, was down to under a minute and the reorientation period was 5 min vs. the prior 30 min.
Omission of DXM in the evening frequently resulted in a seizure in the morning.
Increasing the dose to three times 7 mg per day resulted in a more than three-month seizure-free period up to the writing of this report. The only side effect was moderate tiredness.
Animals
(Wong, 1988) – DXO and DXM antagonize NMDARs and inhibit seizures
Magnesium ion assay
Spontaneous ictal epileptiform afterdischargs were blocked in 7/8 slices with concentrations as low as DXO 1 μM. Epileptiform activity never stopped spontaneously in the non drug-treated slices.
With high concentrations of 250 μM DXO, a few minutes of exposure was usually needed to block afterdischarges.
With 100 μM of DXM, activity was similar, with blockade of epileptiform activity in 6/7 slices. DXM did not appear as effective as DXO.
NMDA-induced intracellular and multi-unit responses in slices
It appears the agents block NMDAR and prevent NMDA-induced depolarizations without altering intrinsic membrane properties. NMDA-evoked depolarizations were blocked by topical applications of DXO 250 μM or DXM 1 mM.
COI: Supported by NIH grants and the Morris and Pimley Research Funds.
(Tortella, 1986) – DXM has anticonvulsant properties
Diphenylhydantoin caused a dose-dependent protection against seizures.
DXM also protected against induced generalized seizures, though it was only half as potent. DXM was longer-acting as an anticonvulsant than diphenylhydantoin.
A subthreshold dose of DXM was able to potentiate the beneficial properties of diphenylhydantoin when given simultaneously. DXM lowered the ED50 3-fold.
Studies with other non-opioid antitussives were conducted with carbetapentane (which has high affinity for the DXM site) and noscapine (which lacks high affinity for the DXM) site.
Like DXM, carbetapentane is an effective anticonvulsant, while noscapine is not, even at the highest dose tested.
COI: Thanking Drs. L.E. Bingenheimer (Wallace Labs.), R.G. Kuntzman (Hoffmann-La Roche) and M.I. Gluckman (Warner-Lambert) for providing carbetapentane, dextromethorphan and diphenylhydantoin, respectively. Also thanked Fisons Corporation for the gift of noscapine.
Local Anesthesia
DXM and its metabolites DXO and 3-methoxymorphinan have local anesthetic properties in rats (Hou, 2006).
(Hou, 2006) – DXM, 3-methoxymorphinan, and DXO are local anesthetics in rats
Male rats.
Results
Mean ED50 for motor, proprioception, and nociception measures (drugs injected into the sciatic notch on the left hind limbs of rats)
Lidocaine: 2.53 mg/kg
DXM: 3.72 mg/kg
3-methoxymorphinan: 6.68 mg/kg
DXO: 14.19 mg/kg
At 6.7 mg/kg, DXM and lidocaine were both effective local anesthetics. DXM produced 71-83% blockade (depending on the measure evaluated), while lidocaine produced 100% blockades.
At high doses, all drugs were capable of producing complete sciatic nerve blockades of motor function, proprioception, and nociception.
COI: Not reported
Rett Syndrome
A study of 38 patients with 2.5 or 5.0 mg/kg per day of DXM found it did not offer a significant reduction in EEG spike count, but it did significantly lower seizure activity and it improved MSEL receptive language scores at 5.0 mg/kg (Smith-Hicks, 2017). A measure of behavioral functioning also showed improvement. This suggests DXM can dose-dependently improve some aspects of the disorder, such as seizures, hyperactivity, and receptive language.
(Smith-Hicks, 2017) – DXM does not improve EEG spike counts in Rett Syndrome, though it does improve some secondary outcome measures
Background
Rett syndrome is defined by mutations in the MECP2 gene. It leads to repetitive stereotyped hand movements, seizures, and chaotic breathing. The symptoms are consistent with excessive excitatory activity in the brain and higher levels of glutamate in CSF have been found in girls with the condition.
Girls aged 2 to 14.5 years with Rett syndrome were studied.
38 patients were randomized to 0.25 mg/kg/d, 2.5 mg/kg/d, or 5.0 mg/kg/d of DXM.
0.25 mg/kg/d was used as a pseudo placebo dose, while 2.5 mg/kg/d was a middle dose, and 5.0 mg/kg/d had been used in earlier studies.
Safety
All patients tolerated the drug without hematologic, liver, electrolyte, or ECG abnormalities. Patients also denied dizziness, skin rash, type 1 diabetes, drowsiness, urinary retention, ataxia, fatigue, dystonia, nystagmus, agitation, persisted nausea, vomiting, increased liver enzymes, or slurred speech.
Results
EEG spikes
There was no difference in EEG spike count distribution for any follow-up visit and no significant changes in count between the two visits for each dose.
Clinical seizures
There was a significant reduction in seizure activity.
Cognitive function
Compared to the 0.25 mg/kg/d dose, the 5 mg/kg/d dose was associated with a significant increase in MSEL receptive language scores of 6.1 points.
The 2.5 mg/kg/d group had a 2.5 point increase compared to the 0.25 mg/kg/d group, but this was not significant.
The dose had a significant association with MSEL receptive language score at follow-up.
There was no significant impact on MSEL expressive language score.
For the VABS communication score, there was no significant improvement.
Behavioral functioning
There was a significant decline in (improvement) in the total ABC score at the 2.5 mg/kg dose and the ABC hyperactivity subscale at the same dose, but no improvement at the remaining doses. There was a non-significant improvement on the SSI (social interaction) subscale.
CGI
Based on the RSSS score between baseline and the second treatment visit, there will be no significant improvement with either dose.
COI: None. Funding came from government and non-corporate sources.
DXM may improve cognition and seizure frequency in people with excess glycine activity caused by a deficiency in the enzyme system responsible for breaking down glycine, though the evidence for its efficacy is small (Bjoraker, 2016). Glycine operates partly through NMDARs.
(Bjoraker, 2016) – Early DXM and benzoate treatment appears to improve outcomes in attenuated nonketotic hyperglycinemia
This study involved families with two siblings both affected by attenuated nonketotic hyperglycinemia. The first sibling was treated late and the second sibling was treated early. The primary outcome was overall neurocognitive ability.
There were 4 families. The first child was diagnosed and treated after 2-6 months, while the second was diagnosed prenatally or neonatally and treated effectively from the first week with both DXM and benzoate.
Results
Children given treatment (DXM was equal to or greater than 3 mg/kg/d for at least the first 2 years) in the first week of life progressed substantially better. This could be seen with cognitive ability, communication skill, and adaptive skill measures, but not on emotional and behavioral scales. Almost all patients had chorea and hyperactivity regardless of treatment.
In each family, the second sibling who had been treated earlier achieved milestones earlier and acquired more skills.
Seizures were less frequent and less severe in the second sibling in 3/4 families.
COI: Not reported
Developmental Disability
A man with severe developmental disabilities caused by congenital rubella failed to respond to many treatments but did respond to DXM 120-180 mg/d, with a significant reduction in aggression, injurious behavior, overactivity, and sleep problems (Welch, 1992). He maintained low levels of self-injurious behavior and aggression during a 16-month follow-up period.
(Welch, 1992) – Significantly improved symptoms of treatment-refractory mental disorder in a patient with severe developmental disability.
25-year-old male with severe developmental disabilities caused by congenital rubella.
Symptoms included (beginning in early childhood) severe overactivity like rocking, hyperventilation, hyperextension of his trunk, and self-stimulation; and irritability. He also had severe aggression and self-injurious behavior, and he had chaotic sleeping patterns.
Failed to respond to a variety of behavioral and psychopharmacological treatments, including haloperidol, thioridazine, chlorpromazine, imipramine, hydroxyzine, carbamazepine, propranolol, and clonazepam.
During a trial of propranolol, he was given DXM cough syrup liquid for 10 days for a URI. The dose during that time was 120 mg/d.
Unexpectedly, he had a marked decline in maladaptive behavior. He was therefore started on Delsym. He was given 60 mg twice daily, while propranolol was discontinued.
Treatment with DXM led to an immediate and dramatic response, with a marked decline in aggression, injurious behavior, overactivity, and sleep problems. After 60 days, the dose increased to 90 mg twice daily due to maladaptive behavior starting to increase.
During a 16-month follow-up period, he maintained low levels of self-injurious behavior and aggression.
COI: Not reported
Autism
DXM 60 mg/d was significantly effective in a 10-year-old with autism, anxiety, and developmental disorder (Woodard, 2005).
(Woodard, 2005) – DXM substantially improved the behavioral symptoms of autism in a single case.
10-year-old male with autism, pervasive developmental disorder, and generalized anxiety disorder.
Treatment with sertraline for 13 months and citalopram for 2 months was not effective. At the start of DXM the child was receiving 0.5 mg twice daily of guanfacine for a 3-month period; this was continued at the same dose during the DXM trial.
Dose: 30 mg twice daily.
Results
Baseline phase: Average daily rate of leaving the classroom was 0.54 incidents/d, and the average daily rate of tantrum was 1.46 incidents/d.
First treatment phase: Average rate of 0 incidents/d for both types.
Second baseline phase: Average rate of leaving the classroom was 0 incidents/d and the rate of tantrum was 0.75 incidents/d.
Second treatment phase: Average rate of 0.09/day for leaving the classroom and 0/day for tantrums.
Parents and teachers reported a distinct improvement during the first treatment phase. The patient had fewer anxiety-related problems, coped more easily with behavioral consequences, became more cooperative, and began to show empathy. When medication was discontinued, anecdotal reports show behavior immediately worsened.
COI: Not reported
Methylmercury Toxicity
In animals, DXM was found to be protective against methylmercury toxicity, which involves glutamate-mediated neurotoxicity (Feng, 2014). It significantly reduced oxidative damage, reduced apoptosis levels, and altered glutamate levels, without changing the amount of mercury in the cerebral cortex.
(Feng, 2014) – DXM is protective in rats against methylmercurcy neurotoxicity
Rats
Groups
Control
Methylmercurcy (4 or 12 μM/kg) injected IP
DXM pretreatment (SC 13.5 μM/kg IP 2 hours before 12 μM/kg MeHg)
Results
Effects of MeHg and DXM pretreatment on total Hg levels in cerebral cortex
Concentration-dependent and significant increase in total Hg content in the 4 and 12 μM/kg MeHg groups. Hg levels with DXM pretreatment were not significantly different from those when only given 12 μM/kg MeHg.
Effects of MeHg and DXM pretreatment on glutamate metabolism in the cerebral cortex
Glutamate and glutamine changed dose-dependently with MeHg administration. The max changes occurred with 12 μM/kg, leading to glutamate increasing by 60.14% and glutamine decreasing by 42.86%.
In contrast, glutamate levels decrease 13.27% and glutamine levels increased 43.75% with DXM pretreatment compared to the MeHg group.
Also, glutamine synthase activity decrease by 61.02% and phosphate-activated glutaminase activity increased 105.22% in 12 μM/kg MeHg group. But glutamine synthase activity increased by 45.25% while phosphate-activated glutaminase activity decreased 24.40% in the DXM pretreatment group vs. those only receiving MeHg.
Effects of MeHg and DXM pretreatment on nonenzymatic and enzymatic antioxidants in the cerebral cortex
NPSH content and SOD and GSH-Px activities decreased in a dose-dependent manner with MeHg. The max decrease was with 12 μM/kg, leading to 37.7%, 58.37%, and 49.20% less activity, respectively.
In contrast, NPSH content and SOD and GSH-Px activities elevated 30.15%, 50.66%, and 57.74% with DXM pretreatment vs. 12 μM/kg MeHg only.
Effects of MeHg and DXM pretreatment on oxidative damage in the cerebral cortex
MeHg
Dose-dependent increase in MDA and protein carbonyl contents, with a maximize rise of 64.60% and 175.11%, respectively, after 12 μM/kg. Dose-dependent decline in protein sulfhydryl content. Induced the appearance of lots of 8-OHdG-positive cells possessing an 8-OHdG-immunopositive cell nucleus. Dose-dependent rise in IOD.
DXM + MeHg
VS 12 μg/kg MeHg only group: MDA and protein carbonyl contents decreased by 20.16% and 31.50%. While protein sulfhydryl content increased by 25.23%. The number of 8-OHdG-positive cells was significantly lower. IOD around the cerebral cortex decreased significantly.
Effect on intracellular free calcium in the cerebral cortex
MeHg
Concentration-dependent rise in free calcium.
DXM pretreatment
Partial decrease in calcium levels compared to the 12 μM/kg MeHg group
Effect on intracellular ROS in the cerebral cortex
MeHg
Dose-dependent decline in DCF fluorescence intensity
DXM pretreatment
DCF fluorescence intensity decreased by 36.42% compared to the 12 μM/kg MeHg group.
Effect on apoptosis levels in the cerebral cortex
MeHg
Dose-dependent increase in apoptosis rates
DXM pretreatment
Significantly fewer apoptotic cells
Effect on NMDAR mRNA and protein expression in the cerebral cortex
MeHg
Significant downregulation in NMDAR mRNA expression.
DXM pretreatment
Significant upregulation of NR1 and NR2A mRNA compared to 12 μM/kg MeHg alone, though there was 1.13% downregulation of NR2B mRNA expression.
Effect on glutamate transporters and protein expression
MeHg
Downregulation of glutamate transporter mRNA expression. Downregulations of GLAST and GLT-1 mRNA expression by 35.64% and 25%, respectively.
DXM pretreatment
GLAST mRNA expression was upregulated significantly while GLT-1 expression was upregulated nonsignificantly.
COI: No conflicts of interest. Work was supported by grants from the National Natural Science Foundation of China.
Endothelial Function and Inflammation in Smokers
A double-blind trial of 40 participants found 60 mg of DXM could improve endothelial function, antioxidant capacity, and inflammation in heavy smokers over a 6-month period (Lie, 2008).
(Lie, 2008) – DXM can improve endothelial function, inflammation, and oxidative stress in male heavy smokers
Double-blind trial with 40 participants. Either given DXM 60 mg oral once daily after breakfast or placebo. 6-month study period
Results
Endothelial function was improved by DXM
Baseline endothelial function was significantly impaired (as measured by flow-mediated dilation method) among habitual smoking groups.
At the end of the study period, there was significant improvement in function in the DXM group, but there was no significant difference in the placebo group.
Changes in nitroglycerin-mediated dilation were not significant in either group, indicating an endothelial-dependent vasodilation improvement with DXM treatment.
DXM significantly increased plasma concentrations of glutathione peroxidase. No significant change was seen in the placebo group. And urinary excretion of 8-PGF2a significantly decreased in the DXM group.
The effects of DXM on plasma VWF and PAI-1 were not significant.
DXM treatment resulted in a clear, dramatic time-related decrease in the level of hs-CRP, decreasing it by about 50% at the end of the study period. Likelise, serum levels of sPLA2, MMP-3, IL-6, and TNF-α RII were also significantly reduced by study end in the DXM group, while remaining stable in the placebo group.
COI: None. This study was supported in part by the Ministry of Education Program for Promoting Academic Excellence in Universities under grant number 91-B-FA09-2-4, and by grants NSC 95- 2752-B-006-003-PAE, NSC 95-2752-B-006-004-PAE and NSC 95-2752-B-006-005-PAE from the National Science Council, Executive Yuan, Taipei, Taiwan. P.-Y. Liu is a recipient of Scientist Physician Award Grant from National Health Research Institute from Taiwan. This study was also support by the Research Grant NCKUH-9702028 from National Cheng Kung University Hospital in 2008.
Chemistry
DXM is a member of the morphinan class of compounds; however, it is specifically the dextrorotary isomer of 3-methoxy-N-methyl-morphinan, which is the opposing chirality to that seen in the structures of morphinan class opioids. The complementary levorotatory isomer, levomethorphan, and its major metabolite, levorphanol, do exhibit significant activity at various opioid receptors.
DXM is primarily metabolized via demethylation of the methoxy group to form dextrorphan, though demethylation can also occur at the amine of either compound to give 3-methoxymorphinan and 3-hydroxymorphinan as additional metabolites
Pharmacology
DXM and its metabolite DXO interact with many targets, most notably σ1, the serotonin transporter (SERT), and NMDAR. DXM is often viewed as a ketamine-like dissociative and its NMDAR antagonism is emphasized, but its action at σ1 and SERT is greater. NMDAR antagonism likely does play a role in the substantial non-medical effects of DXM and in some of its medical efficacy.
At NMDAR it binds to to the same site as PCP and ketamine.
σ1 agonism could contribute to the muscle tension, tachycardia, tachypnea, and mydriasis seen with DXM. Because sigma activity is also linked to motor function, it’s speculated to play a role in the well-known movement effects of DXM, such as “robo walking” or “zombie walking.”
DXO is usually present at a higher level than DXM, making it the primary active drug followed DXM administration. A lot of research in humans has begun to use DXM alongside quinidine to inhibit its metabolism to DXO, which then shifts the dominant drug to DXM itself. Naturally, poor metabolizers can be exposed to much higher DXM plasma levels than normal metabolizers.
Important affinity values (Taylor, 2016):
SERT: 40 nM (DXM) and 484 nM (DXO)
σ1: 150 nM (DXM) and 118 nM (DXO)
NET: 6000 nM (DXM) and 6200 nM (DXO)
NMDAR: 2120 nM (DXM) and 892 nM (DXO)
Adrenergic α1D: 830 nM (DXM)
Adrenergic α1A: 3000 nM (DXM)
σ2: 11,060 nM (DXM) and 11,325 nM (DXO)
5-HT1B/D: 61% at 1000 nM (DXM) and 54% at 1000 nM (DXO)
Adrenergic α2: 60% at 1000 nM (DXM)
Histamine-1: 95% at 1000 nM (DXO)
DXO also differs from DXM in that it shows significant competition for muscarinic acetylcholine receptors and histamine H1 receptors at 1 μM (Werling, 2007), compared to no competition from DXM. Those properties could play a role in the effects of DXM/DXO at recreational/nonmedical doses.
Very high concentrations of DXM and DXO can function as calcium channel antagonists. The IC50 values are upwards of ~50 μM, which means they are likely too high to matter (Kamel, 2008 ; Carpenter, 1988). Both drugs also antagonize α3β4 nicotinic receptors. (Taylor, 2016 ; Hernandez, 2000).
Brain levels of DXM and DXO are much higher than serum levels (Steinberg, 1996).
DXM also impacts the HPA axis and can increase steroid hormones like ACTH and corticosterone, the dominant corticosteroid in rats (Pechnik, 2004). The study demonstrating this used rats, so if the effect also exists in humans, DXM likely raises cortisol, the dominant corticosteroid in humans.
(Pechnick, 2004) – DXM and DXO impact the HPA axis, shown by increases in ACTH and corticosterone in rats.
Male rats. SC injections.
Results
DXM and DXO acutely increased plasma ACTH. DXM’s effect was greater at 30 minutes, while there was a more delayed rise from DXO, which had a larger rise at 60 min.
Both drugs also increased plasma corticosterone. Again, DXM had a more rapid effect, but DXM’s effect was lower than DXO’s by 60 minutes.
Based on dose-response data (from 3.0 – 30 mg/kg), only the highest 30 mg/kg dose of either drug was significantly effective.
For comparison, levorphanol (3.0 and 10.0 mg/kg) more potently increased ACTH and corticosterone.
60 min post-administration, the DXO level produced from DXM administration was just 3% that of DXM, indicating the concentration is too low to be responsible for the effects of DXM.
Naloxone
Naloxone at 2 mg/kg was able to block the ACTH and corticosterone increase triggered by levorphanol (a known opioid agonist), but it didn’t affect the changes from DXM and DXO.
COI: Not reported
Pharmacokinetics
The metabolism of DXM is very important to its pharmacology. CYP2D6 catalyzes the transformation of DXM to DXO, which retains a substantial amount of activity and is a more potent NMDAR antagonist. People with faster 2D6-dependent metabolism (i.e. either normal extensive metabolizers or ultrarapid metabolizers) could receive greater dissociative effects.
DXM (demethylation via CYP2D6) –> DXO (demethylation via CYP3A4) –> 3-hydroxymorphinan
DXM (demethylation via CYP3A4) –> 3-methoxymorphinan (demethylation via CYP2D6) –> 3-hydroxymorphinan
30 mg DXM yields a serum concentration of 0.21 to 7.62 ng/mL for DXM. The Cmax of DXO in extensive metabolizers can be up to 100x higher. (Pope, 2004).
Drugs that could lower 2D6-dependent metabolism include: clomipramine, bupropion, paroxetine, duloxetine, fluoxetine, haloperidol, methadone, quinidine, amiodarone, metoclopramine, ritonavir, mibefradil, chlorpheniramine, and cimetidine.
Grapefruit juice can reduce the amount of CYP3A4-dependent metabolite production, but it does not significantly change the plasma level of DXM, at least at 10 mg DXM (Strauch, 2009). Possibly from P-glycoprotein inhibition or from CYP3A4 inhibition, grapefruit juice and seville orange juice were found to increase the bioavailability of DXM (Marco, 2002).
Black cumin seed extract significantly inhibited the formation of DXO and 3-methoxymorphinan from 30 mg of DXM, which fits with black cumin seed’s CYP2D6-inhibiting property (Al-Jenoobi, 2010). Grape seed extract, which can inhibit CYP2D6 in vitro, did not significantly change the pharmacokinetics of DXM 30 mg when given at 300 mg/d (Goey, 2013).
History
1950s
The preparation of DXM was patented in the US in 1954 by Hoffmann-La Roche, a Swiss pharmaceutical company, though it was synthesized and investigated earlier (Cass, 1953).
Research in the early 1950s found it had antitussive properties in animals. It was then approved for that use by the FDA in 1958, allowing DXM to be sold as a non-prescription cough suppressant. It became a popular alternative to codeine.
From 1954 to 1964, the US federal government was involved in a program to find a non-addictive codeine alternative. This research was part of a project known as MKPILOT and the work was completed at the Addictive Research Center, which was part of the US Public Health Service Hospital in Lexington, Kentucky. A researcher at that facility tested ~800 drugs on addicted patients, one of which was DXM. The CIA transferred at least $282,215 to the Office of Naval Research as part of this program. The CIA’s interest in the research was “classified secret and is not to be revealed.”
1960s and 1970s
Recreational use was reported by the mid-1960s (Degkwitz, 1964). McCarthy (1971) reports it was used recreationally by young people near Brisbane, Australia around 1968 to 1969. They reported perceptual changes, visual hallucinations, and an altered sense of time. A typical dose was ~1 bottle (100 mg) and it was often mixed to cover up the unpleasant taste.
A tablet form of pure DXM, Romilar, was withdrawn from the market in 1973 due to increasing use within the counterculture.
DXM was excluded from the 1970 Controlled Substances Act to keep it from being treated as an analog of the Schedule 2 substance levomethorphan, which has opioid activity.
1980s
In the UK, there were no published reports of DXM misuse until at least 1986 and the UK Home Office drugs branch along with British manufacturers of the drug were not aware of any cases of misuse in the country (Fleming, 1986).
Utah saw a substantial level of adolescent nonmedical use of DXM in the 1980s, leading to the voluntary placement of DXM products behind pharmacy counters.
In 1986, the Swedish National Board of Health and Welfare forced DXM into prescription drug status due to teenage abuse of the substance. Teenagers around the country had begun using it recreationally earlier in the decade.
1990s
The availability of geltab products may have contributed to a rise in recreational use since they provided an alternative to the unpleasant taste of cough syrups.
In 1990, the Pennsylvania Health Authorities and the FDA both held hearings about DXM that were driven by reports of nonmedical use.
Usenet became an active online forum for discussion about DXM’s properties and how to extract it from syrups (Morris, 2014). There were also posts about online chemical vendors selling pure DXM HBr as early as 1996.
2000s
A significant rise in the nonmedical use of DXM by adolescents in California was reported from 1999 to 2004 (Bryner, 2006). The frequency of reports increased 10-fold from 48 in 1999 to 478 in 2004. Similar trends were seen nationwide. Most cases only led to minor or moderate effects, according to data from poison control centers. Typically it resulted in no more than altered mental status, tachycardia, hypertension, mydriasis, agitation, and GI effects.
Texas rave parties reportedly featured intentional and unintentional DXM use as an alternative to MDMA in the early 2000s, according to a report from InteliHealth (McFee, 2000). Fitting with this report, Baggott (2000) found DXM was a common substance in the MDMA/ecstasy market, with 21% of pills analyzed by DanceSafe between February 1999 and March 2000 containing the substance.
Texas poison control centers reported a rise in abuse/misuse between 1998 and 2002, according to the Gulf Coast Addiction Technology Transfer Center. A large portion of those cases had come to involve Coricidin HBP specifically.
A large-scale drug bust by the DEA, known as Operation Web Tryp, reduced the online availability of DXM powder in 2004 (Morris, 2014).
Visits to US emergency departments related to the nonmedical use of DXM products doubled from 4,000 to 8,000 between 2004 and 2008, according to the Drug Abuse Warning Network (DAWN). Data from the 2006 NSDUH survey of 67,802 people in the US found 4% of adolescents reported using OTC cough medications recreationally, with 2% reporting past-year use (Ford, 2009). This was compared to 10% reporting binge drinking and 13% reporting cannabis use.
In early 2006, a survey given to a sample of 12th grade Ohio students found 4.9% reported lifetime use of DXM (Falck, 2006). 3.7% had used it in the past year.
2010s
The FDA approved DXM/quinidine in 2010 for pseudobulbar affect. That was followed by approval from the European Medicines Agency in 2013.
In the same year, the FDA’s Drug Safety and Risk Management Committee voted 15-9 against scheduling DXM despite its nonmedical use (Traynor, 2010). The committee members felt its economic and public health benefits outweighed the downsides of unscheduled status. Placement in Schedule 5 had been proposed, which would have permitted non-prescription use under federal law, but FDA officials were uncertain about how available DXM would be in states with more restrictive laws than the federal statute, since some states mandate prescriptions for Schedule 5 drugs.
The DEA considers it a drug of concern because of its widespread availability to adolescents and young adults. According to the Consumer Healthcare Products Association (CHPA), ~90% of nonprescription cough medicines contain DXM and 133 million packages of nonprescription DXM-containing products were sold in the US in 2009.
In Spring 2011, an outbreak of DXM hospitalizations due to the use of paracetamol-containing products was reported in British Columbia. First Nations teens used up to 36 tablets, exposing them to 540 mg DXM and 1800 mg paracetamol, a toxic amount.
California banned the sale of DXM to minors without a prescription in 2012. Other states have similar restrictions in place.
A survey of community pharmacists in Scotland found DXM misuse does not appear to be a major or growing problem, even though over 80% of pharmacists reported OTC product misuse in general is a problem in their region (Wright, 2015).
Legality (as of June 2018)
United States: Unscheduled; sold OTC
Australia: Pharmacy medicine; sold OTC
Canada: Unscheduled; sold OTC
United Kingdom: Pharmacy only; Available without prescription
Safety
DXM is rarely lethal on its own and far more often causes acute psychological problems than physical health issues. Even though most DXM-containing products include other substances, such as guaifenesin and chlorpheniramine, fatalities still aren’t very common. Lethality is of greater concern when combining it with other serotonergic substances.
At common to strong recreational doses, heart rate and blood pressure increase significantly, such as an average of 20 mmHg for systolic blood pressure and 20 bpm for heart rate at 400 mg (Carbonaro, 2017). Systolic blood pressure is more affected than diastolic. This increase is usually greater than from psychedelics, though it’s not dangerous in an otherwise healthy person.
When hundreds of milligrams or more are used, the primary concerns are psychological problems (e.g. mania, psychosis, hallucinations, agitation), drowsiness, hypertension, and tachycardia. Other symptoms include ataxia, urinary retention, mydriasis, nystagmus, stupor, and coma. Seizures and hyperthermia are rarely reported and there are even fewer cases where impaired respiration has been a problem.
A review of data from US poison control centers found 44,206 cases of intentional “abuse” from 2000 to 2010 (Wilson, 2011). 17 fatalities were reported, with five coming from single-product exposures, namely Coricidin Cough and Cold (n=3), Zicam (n=1), and Mucinex (n=1). There were 4704 single-product cases in which DXM was the only active ingredient. Seizures (n=38), coma (n=25), dystonia (n=22), respiratory arrest (n=1), and cardiac arrest (n=1) were infrequently reported.
Wilson (2011) found multi-substance exposures accounted for 21.4% of all DXM abuse cases, with the most common coingestants being ethanol, cannabinoids, antihistamines, benzodiazepines, opioids, cocaine, and MDMA. The risk of a severe outcome was increased the most in cases involving opioids, benzodiazepines, cocaine, or ethanol.
Fatalities
Fatalities do infrequently occur and it appears possible to die just from taking DXM, but at a dose much greater than the typical recreational range. When it is deadly, it may disrupt respiration, though the exact mechanism of lethality is not understood.
(Shafi, 2016) – Fatalities from DXM combined with a variety of other drugs
Background
In Pakistan there were over 50 deaths related to DXM cough syrup from two incidents in 2013.
This report covers the deaths of 19 subjects who used DXM cough syrup recreationally in combination with benzodiazepines, opioids, cannabinoids, chlorpheniramine, and ethanol.
Incident 1 – Lahore, Pakistan
Over 30 deaths in Lahore city due to ingestion of cough syrup with DXM.
Autopsy specimens from 12 males (18 to 45 years old) were analyzed. The results revealed an opioid-type overdose with pulmonary and cerebral edema, congested lungs and other airways, and no signs of trauma.
Toxicology
Peripheral blood concentration for DXM was 7.3 to 41.7 mg/L
Chlorpheniramine was also detected but not quantified.
All subjects tested positive for opioids, 8 for cannabinoids, and 2 for benzodiazepines via immunoassay.
Cause of death: Acute DXM intoxication
Incident 2 – Gujranwala, Pakistan
20 DXM-related deaths linked to the abuse of an OTC cough syrup containing DXM manufactured by another National pharmaceutical industry.
7 postmortem specimens were analyzed. Autopsy again showed opioid-type overdose with significant pulmonary edema.
Toxicology
4.2 to 92.6 mg/kg DXM in the liver and 9.9-349.6 mg/L in gastric contents.
All tested positive for opioids, 3 for cannabinoids, and 2 for benzodiazepines via immunoassay.
COI: None
(Logan, 2009) – Five fatalities
Cases involving the purchase of DXM in powder form online then overdoses leading or contributing to fatalities.
All incidents were later traced to the same internet supplier of DXM, “Chemical API,” a chemical resale company in Indianapolis, Indiana. They were buying the drug in bulk from India, repacking it, and selling it online. The two individuals behind the company later pleaded guilty to 3 counts of introduction of misbranded drugs into interstate commerce and were sentenced to 77 months in prison.
Also, the individual in Virgnia who ordered the DXM and provided it to the teenager who died was convicted of involuntary manslaughter.
Incident 1 – Bellingham, Washington
17-year-old male and 19-year-old male died after obtaining DXM over the internet for recreational use. They had previous experience; started with cough medicine preparations.
Found dead near a clear bag of white powder labeled “dextromethoprhan Hbr 100 grams.”
Autopsy showed two healthy individuals with non-specific but common findings associated with opioid-type overdose: pulmonary edema, cerebral edema, presence of frothy foam in oropharynx and major airways, and no signs of trauma or antecedent natural disease.
Toxicology
17-year-old: 3230 μg/L (heart blood)
19-year-old: 1890 μg/L and diphenhydramine at 20 μg/L (heart blood)
Both cases determined to be acute DXM intoxication, leading to accidental death. Lack of other significant drugs in the cases heavily implicate DXM.
Law enforcement investigation indicated they obtained a large quantity for the purpose of potential distribution at the local high school. A third-party teen had purchased the DXM for $205. They then reportedly repackaged the powder into capsules. At least 3 other nonfatal overdoses were linked to those capsules.
Incident 2 – Danville, Virgonia
19-year-old male. Only significant pathology finding was pulmonary edema.
Toxicology
DXM: 1300 μg/L in iliac blood and over 20,000 μg/L in urine.
Also positive for alprazolam in blood at under 10 μg/L.
Ruled an accidental drug toxicity caused by DXM.
Incident 3 – Cape Coral, Florida
Two 19-year-old males found dead
Toxicology
DXM: 950 μg/L and 3080 μg/L (iliac blood)
Diphenhydramine: 264 μg/L and 238 μg/L (iliac blood; therapeutic range of 30-50 μg/L)
Autopsies showed no underlying natural disease.
Cause of death was drug intoxication from DXM combined with diphenhydramine.
COI: Not reported
(Marinetti, 2005) – Cases of infant deaths associated with cold medications
Case 1
12-month-old infant. A few days prior to death, treatment began with Children’s Tylenol Plus-Cold and Cough
Found cold and unresponsive. Medical history remarkable for Down’s Syndrome and the infant was dependent on a feeding tube.
Cause of death: Klebsiella pneumonia sepsis, due to Klebsiella pneumonia. Toxic levels of Children’s Tylenol Plus-Cold and Cough contributed.
Toxicology (cavity blood)
DXM: 0.55 mg/L
Ephedrine: 0.39 mg/L
Pseudoephedrine: 1.5 mg/L
Paracetamol: 117 mg/L
Case 2
8-month-old infant. Given Tyenol then found face-down and unresponsive in crib.
Investigation found a 4-ounch bottle of Children’s Tylenol Plus-Cold and Cough cherry flavor on the kitchen counter with approximately 1/2 ounce remaining.
Cause of death: Positional asphyxia with multiple drug intoxication contributing.
Toxicology (peripheral blood)
DXM: 0.37 mg/L
Ephedrine: 0.14 mg/L
Pseudoephedrine: 1.1 mg/L
Chlorpheniramine: 0.08 mg/L
Paracetamol: 6.6 mg/L
Case 5
2-month old infant. Found unresponsive and then pronounced dead upon hospital arrival.
Cause of death: Acute intoxication with DXM, ephedrine, pseudoephedrine, and carbinoxamine.
Toxicology (heart blood)
DXM: 0.04 mg/L
Ephedrine: 0.50 mg/L
Pseudoephedrine: 2.2 mg/L
Paracetamol: 16 mg/L
Carbinoxamine: 0.08 mg/L
Case 8
3-month-old infant. Found dead in bed cosleeping with mother. Had been medicated with Infant Tylenol and OTC cold remedies.
Infant’s doctor suspected the death was due to overdose with OTC cold medications, but the coroner ruled it Sudden Infant Death Syndrome.
Toxicology (heart blood)
DXM: 0.03 mg/L
Ephedrine: 0.09 mg/L
Pseudoephedrine: 2.9 mg /L
Paracetamol: 24 mg/L
Levorphanol: 0.04 mg/L
Case 9
3-month-old infant. Found unresponsive.
Given the pediatric formulation of Tylenol Cough and Cold.
Neither the autopsy nor the cause of death are known.
Toxicology (femoral blood)
DXM: 0.04 mg/L
Ephedrine: 0.4 mg/L
Pseudoephedrine: 0.52 mg/L
Paracetamol: 1.7 mg/L
Case 10
5-month-old infant. Had been given an OTC cold medication containing DXM.
Found unresponsive and quickly pronounced dead.
Cause of death: Acute multiple drug intoxication.
Investigation revealed the infant’s 3-year-old and 4-year-old siblings were regularly given OTC cold medications to sedate them, leading to their removal from the home. An investigation did reveal DXM in the blood and urine of these children.
Toxicology (cavity blood)
DXM: 0.09 mg/L
Ephedrine: under 0.10 mg/L
Pseudoephedrine: 1.4 mg/L
Paracetamol: 6 mg/L
Carbinoxamine: 0.07 mg/L
Metoclopramide: 0.67 mg/L
COI: Not reported
(Boland, 2003) – Cold medication death in infant
2-month-old female. Had been given Tylenol. Found unresponsive and pronounced dead at the scene.
Toxicology positive for brompheniramine, DXM, and pseudoephedrine. Those were in postmortem blood and liver specimens.
Toxicology results indicate the child was given significantly more OTC cold medications than suggested.
(Yoo, 1996) – Fatalities stemming from the combined use of DXM and zipeprol
Zipeprol is a centrally active cough suppressant with mucolytic, antihistamine, and antimuscarinic properties. It’s been abused for its hallucinogenic properties. It’s reportedly been known to produce an opioid-like euphoria with large doses and its abuse has become common among young people in South Korea. There’s a growing tendency to use it alongside DXM to obtain a stronger hallucinogenic effect.
This report involves 9 fatalities featuring both drugs.
Postmortem concentrations
Zipeprol
Blood: Range from 1.3 to 28.6 μg/mL (comparable to levels from a prior report of 23 zipeprol fatalities)
DXM
1.1 to 18.3 μg/mL (lower than the levels from another study that had 5 DXM-involved fatalities).
COI: Not reported
(Kintz, 1992) – DXM death with terfenadine
22-year-old female found dead at home. DXM found in the toxic range.
Toxicology
Whole blood
DXM: 5.09 mg/L
DXO: 1.40 mg/L
Terfenadine: 7.22 mg/L
COI: Not reported
(Rammer, 1988) – Two fatality cases involving DXM
Case 1
18-year-old female found dead near two empty bottles of Extuson, a DXM product in tablet form. Two weeks prior she had attempted suicide with 50 tablets of the same preparation.
Toxicology
Blood from femoral vein
DXM: 9.2 μg/g
DXO: 2.9 μg/g
DXM to DXO ratio of 3.17
Liver
DXM: 31.2 μg/g
DXO: 11.5 μg/g
DXM to DXO ratio of 2.79
Case 2
27-year-old male found dead in bed.
Toxicology
Blood from femoral vein
DXM: 3.3 μg/g
DXO: 1.5 μg/g
DXM to DXO ratio of 7.88
Liver
DXM: 230 μg/g
DXO: 29.2 μg/g
DXM to DXO ratio of 7.88
COI: Not reported
Serotonin toxicity & Problems from other serotonergic combinations
Serotonin toxicity typically comes from using a combination of serotonergic drugs, but sometimes it can occur after taking a single substance. The symptoms can include hyperthermia, diaphoresis, tachycardia, tachypnea, flushing, diarrhea, hypertension, and dyspnea. The mental symptoms include confusion, coma, anxiety, agitation, restlessness, and insomnia.
DXM is implicated in serotonin toxicity due to its inhibition of serotonin reuptake and potential ability to promote serotonin release.
Usually toxicity is only seen with very high doses of at least one of the substances involved, such as a high recreational dose of DXM mixed with a therapeutic dose of an SSRI. Otherwise, those combinations are common (i.e. many people are on serotonergic antidepressants and also take DXM for cold symptoms) and rarely lead to problems.
Serotonin toxicity from DXM appears to involve the 5-HT1A receptor and the induction of PKC-δ in the hypothalamus (Tran, 2016 ; Tran, 2016).
In other cases serotonin toxicity isn’t seen, but problems still arise from combining multiple serotonergic drugs. Issues have been reported when combing DXM with SSRIs, TCAs, MAOIs, tramadol, and methadone.
Case Reports
(Okland, 2016) – Patient with psychiatric problems suffering problematic mental effects after large doses of DXM.
29-year-old male. Brought to the hospital after being found disoriented and agitated.
Psychiatric history: Bipolar 1, anxiety, and a prior suicide attempt.
Medications: Buspirone, duloxetine, and lurasidone. He reported inconsistently using those.
He reported frequent cough medicine abuse and had taken 32 capsules of Coricidin Cough and Cold (DXM and chlorpheniramine) prior to admission.
Presented diaphoretic, tremulous, and confused. Vital signs notable for tachycardia and hypertension. Physical exam showed bilateral, inducible clonus at the ankles, with rigidity.
He was only oriented to self and place. He was also verbally aggressive with staff and had to be placed in restraints.
Emergency team concluded his symptoms were consistent with serotonin syndrome. IV fluids and benzodiazepine therapy began; it was also recommended he be discontinued from buspirone and duloxetine due to their serotonergic properties.
He had a good response to fluids and lorazepam over the next two days. But he was anxious and aggressive, requiring security be called multiple times. His status improved during inpatient service and he was discharged within two days of his stay.
On the night of his discharge he was found agitated and confused, striking himself repeatedly in the face with fists. He admitted taking two boxes of cough medicine containing DXM, while denying any other drug/medication use.
COI: Not reported
(Madisi, 2014) – DXM-only serotonin syndrome
52-year-old male with a history of bipolar disorder and prior DXM abuse. He was brought to the ED after being found stiff in a chair and poorly responsive.
Exam: Diahporesis, tremors, agitation, hyperreflexia, altered mental status. ICU admission was required for hypotension and hypoxemia.
Significant lab data: CPK of 18,000 units/L and myoglobin of 16,000 μg/mL, consistent with rhabdomyolysis.
He developed oliguric renal failure.
Urine toxicology was positive for PCP, while all other tox screens were negative. History revealed he had actually ingested 3 bottles of DXM earlier in the day.
Given the rigidity, altered mental status, and diaphoresis, he was diagnosed with serotonin syndrome.
Treatment: Cyproheptadine and supportive therapy, including pressors, intubation, and continuous renal replacement therapy. His symptoms then improved and he was discharged home.
COI: None
(Sethi, 2012) – Case of serotonin syndrome due to sertraline and dextromethorphan
46-year-old male. On sertraline 100 mg/d for 2 years (depression) as well as metformin 500 mg bid and levothyroxine 100 μg daily.
After developing cough, congestion, and insomnia, his PCP recommended OTC medication. So he ended up buying NyQuil containing DXM and in one night he drank 240 mL of the liquid.
Presented to the ED the next day with confusion, shivering, agitation, fever, diaphoresis, stupor, hyperreflexia, and diarrhea. Exam showed 110 HR, BP of 155/89, tachypnea at 24, and hyperthermia at 39.0°C. Mydriasis and hyperactive bowel sounds were shown. Neurologic exam showed hyperreflexia, tremor, and rigidity.
Labs were mostly normal, except for metabolic acidosis and high blood urea nitrogen/creatinine levels.
Diagnosed with serotonin syndrome. He met Sternbach criteria for serotonin syndrome.
Improved with diazepam (1 mg every 4 hours as needed) and IV fluids. Symptoms resolved within 2 day and he was discharged. His sertraline was discontinued and replaced with mirtazapine.
COI: Not reported
(Kinoshita, 2011) – DXM-only serotonin syndrome in an elderly patient
77-year-old male with hepatitis from hepatitis C. He also had chronic renal dysfunction.
4 days prior to admission
Family doctor prescribed DXM tablets at a dose of 45 mg/d to relieve cough. He was not taking SSRIs or MAOIs. After this treatment he began to have involuntary movements in the whole body and could not stand without assistance.
Admission
Vital signs normal. Restless and his voice was tremulous. There was a 4-8 Hz tremor involving the head, neck, shoulders, trunk, and extremities. Symptoms would worsen with movement and were also present while still.
He also had brief, jerky, arrhythmic involuntary movement that was considered to be negative myoclonus.
Patient reported he had experienced the same symptoms after treatment with DXM 5 years earlier. On the basis of this info, the diagnosis was DXM-induced serotonin syndrome.
The symptoms resolved within 3 days of discontinuing the drug.
COI: Not reported
(Monte, 2010) – Case report of serotonin toxicity from DXM and chlorphenamine, along with a literature review
Case report
19-year-old male arrived at ED 12 hours post-ingestion of up to 48 tablets of Coricidin Cough and Cold (each containing 30 mg DXM and 4 mg chlorphenamine; so up to 1440 mg DXM and 192 mg chlorphenamine)
Was agitated and delirious. Vitals: 177/113 BP, 128 HR, respiration of 18, temperature of 38.5°C.
Mydriasis and ocular clonus. Skin was warm and dry; mucous membranes dry. Axillary sweat, bowel sounds present, no urinary retention.
Bilateral inducible sustained ankle clonus.
ECG: sinus tachycardia, normal PR, QRS, and QTc intervals.
As mental status cleared, patient denied any drug use other than Coricidin Cough and Cold.
Sedated with repetitive doses of lorazepam and treated with IV fluids.
Vital signs normalized and mental status cleared over a 6-hour period.
Toxicology (plasma)
DXM: 250 ng/ml
Chlorphenamine: 330 ng/ml
Literature review
Reviewing all English-language case reports of DXM or chlorphenamine-induced serotonin toxicity published through December 2009.
6 cases, including the above one, with serotonin toxicity associated with DXM. 3/6 also involved chlorphenamine.
In 3/6 cases, DXM and chlorphenamine were the only overdosed drugs. Some others involved paroxetine, escitalopram, and sertraline, which have serotonergic effects and could be CYP2D6-inhibiting.
COI: None
(Schwartz, 2008) – Two cases of serotonin syndrome from DXM and SSRIs
Case 1
20-year-old male found confused. Paramedics gave naloxone 2 mg and dextrose for low blood glucose with no effect. He was brought to the ED and found to have a temp of 102°F, he was confused, and tremulous.
Potential medication exposure included aripiprazole, benztropine, escitalopram, and DXM-containing cough medications.
Vitals: temp 38.4°C, respiration 16, BP 150/80, oxygen saturation of 94% on room air.
He was warm, flushed, and had generalized diaphoresis. Pupils were 6 mm and reactive.
Tremulous, lethargic, but easily aroused with incomprehensible speech. Lower extremities were rigid and hyperreflexic, with seven beat clonus at both ankles.
Due to seizure concerns, an EEG was performed and was negative for epileptiform activity.
Drug screen was positive for opioids, cannabis, and PCP (usually a false positive due to DXM). While paracetamol, salicylate, and ethanol were not detectable.
Serum CPK was 327 units/L and white blood count was 14,500/mm3
Treatment: Over a period of 90 min he received lorazepam 6 mg (IV), cyproheptadine 12 mg (oral), and IV fluids. He was then resting without tremor and with a HR of 124.
Within 12 hours he was awake and neurologically normal with a falling creatine kinase. He admitted taking large amounts of DXM-containing cough medications and denied and supratherapeutic use of his medications.
Toxicology (admission levels; serum)
DXM: 950 ng/mL
Citalopram/escitalopram: 23 ng/mL (therapeutic: under 200)
Chlorpheniramine: 430 ng/mL (therapeutic: under 20)
Undectable levels of aripiprazole and benztropine.
Case 2
6-year-old male who was recently started on sertraline. He was found lethargic and confused with an empty bottle of DXM elixir. The estimated exposure was 40 mg/kg of DXM.
Exam at ED: 100.6°F, HR 118, BP 140/69, and respiration 24.
Skin was warm and diaphoretic. Neurologically he was confused and irritable with rigidity and clonus in his lower extremities only. Pupils were delated.
Treatment: Sedation with fentanyl and versed, intubated with airway support, and IV fluids.
He was extubated and neurologically intact within 15 hr of admission.
Toxicology (admission; serum)
DXM: 2820 ng/mL
Sertraline: 12.5 ng/mL (therapeutic: under 200)
Caffeine: 1.4 μg/mL (low)
COI: Not reported
(Forget, 2008) – Life-threatening intoxication from the use of DXM with amitriptyline in a poor CYP2D6 metabolizer
60-year-old male. He was receiving opioids for neuropathic pain and eventually gabapentin, clonazepam, and amitriptyline were also added.
He began taking a DXM preparation containing DXM 15 mg, guaifenesin 50 mg. This was used three times daily. After the 4th dose he became very somnolent and 12 hours later he was admitted into the ED for profound coma.
All analgesic drugs were stopped and his condition normalized 36 hours later.
Genotyping showed he was a poor metabolizer at CYP2D6.
When the drugs were reintroduced (analgesics on Day 1 and then DXM on Day 2) he developed somnolence on Day 3, 30 hours after the first dose of DXM.
Plasma drug concentration analysis showed stable profiles for amitriptyline, nortriptyline, and hydromorphine. But for DXM, there was an accumulation without reaching steady state. A 30 mg dose led to a 4-hour plasma level of 13 ng/mL, whereas a study found that a typical concentration is 5.2 ng/mL after 60 mg.
His concentration kept increasing with following doses and somnolence was noted for plasma concentrations around 100 ng/mL.
COI: Not reported
(Ganetsky, 2007) – Serotonin syndrome after DXM; responsive to propofol
18-year-old male was found unresponsive. He was intubated by paramedics. At arrival in the ED, he was tachycardic, agitated, and diaphoretic. Examination showed mydriasis and ocular clonus.
Muscle tone in his lower extremities was increased, as were patellar and Achilles deep tendon reflexes. He had persistent tremor and inducible, sustained ankle clonus.
HR 132, BP 123/75, and respiration 23, temperature 37.2°C
He was initially sedated with lorazepam 4 mg (IV) then he received a continuous infusion of propofol, which was started at 10 μg/kg per minute, though it had to be increased to 30 μg/kg per minute.
HR declined to 70 and his neuromuscular tone and reflexes quickly normalized.
Three boxes of Coricidin HBP (chlorpheniramine 4 mg and DXM 30 mg) were found in his possessions, two of which were empty.
He was diagnosed with serotonin syndrome.
Propofol was discontinued 2 hours post-presentation. The patient rapidly became agitated and had a return of ocular clonus, tachycardia, lower extremity hypertonia, and clonus. The symptoms resolved when propofol was started again.
10 hours after presentation: Propofol was again discontinued, this time without issue and he was successfully extubated.
The patient admitted to taking 16 tablets, containing 480 mg DXM and 64 mg chlorpheniramine with the goal of hallucinating.
Toxicology (initial; serum)
930 ng/mL, which was considered to be consistent with his reported dose.
COI: One of the co-authors was previously a consultant for Proctor & Gamble. No conflicts listed.
(Kung, 2007) – Serotonin syndrome case apparently stemming from tramadol and DXM.
29-year-old male presented for epigastric pain. He had on-and-off epigastric pain for 3 weeks and had diarrhea three times and vomiting once in the past 2 days.
Exam: temperature 37°C, BP 161/91, HR 136. He was fully alert. Exams of his abdomen, cardiovascular system, and CNS were normal.
Hyoscine (IM) was given along with an antacid (oral). Since the pain didn’t improve, he received tramadol 100 mg (IM) at 1 hr 35 min post-presentation then morphine 2 mg (IV) at 2 hr 55 min.
Metocloprameine 10 mg (IV) was given at 3 hr 40 min
4 hours after presentation he quickly developed irregular, asymmetric twitching of all four limbs. He was also agitated, confused, and not obeying command. He did not have hyperthermia. There was no cyanosis, hypotension, or hypoglycemia. His skin was not dry, but his muscle tone was increased.
ECG showed HR 162, prolonged QTc interval of 552 ms and QRS interval of 104 ms
Patient history from his family revealed multiple medications recently prescribed by a private doctor for flu-like symptoms and abdominal pain. Those included slow-release theophylline, domperidone, promethazine, DXM, paracetamol, hyoscine, and sennoside B.
After the twitching he showed metabolic acidosis, with basically normal liver and renal tests.
Diazepam was given, then midazolam.
Serotonin syndrome was the most likely diagnosis, attributable to DXM, tramadol, and metoclopramide.
COI: Not reported
(Lotrich, 2004) – A case of confusion, increased depression, drowsiness, and impairment possibly stemming from an interaction between DXM and methadone in an elderly patient
83-year-old female. She had a 5-month period of hypersomnia, confusion, and poor eating following brief hospitalization for pneumonia. Several days after hospital discharge she became very confused and began falling down. Yet prior to this she was highly functional, physically and mentally, and socialized actively.
Her confusion did not resolve by changing her antidepressant medication from sertraline to escitalopram.
She was discharged to a nurisng home where she remained unable to care for herself for the ensuing 5 months. Multiple narcotics had been previously prescribed for pain, the most recent being methadone 20 mg/d and hydrocodone/paracetamol as needed.
At the time of the pneumonia, DXM 30 mg with guaifenesin 600 mg twice daily had been started for cough. Despite no record of chronic cough, the medication had not been stopped.
Evaluation in the nursing home: lethargic. Confirmed she had poor appetite, hypersomnia, sadness, hopelessness, and a passive wish to die. No evidence of thought disorder, hallucinations, or delusions. Though she had intermittent episodes of staring for 10 sec at a time, which had been spontaneously reported by the family as well. Her memory was moderately impaired and her attention was markedly impaired.
A decreased in methadone to 7.5 mg/d failed to change her mental status. DXM was discontinued without worsening cough. After 1 week, she was increasingly alert, eating better, and spontaneously reported feeling less confusion. Her cognitive impairment improved over the next 1-2 weeks. After several weeks, her mood and affect were still bright and she had returned to socializing. The methadone dose was then further tapered and discontinued at 2 months.
Discussion
Methadone is a known CYP2D6 inhibitor, which could underlie this apparent interaction. Though prior reports of problems from the combo have not been reported and a study in people receiving methadone maintenance also failed to show problems when concurrently given DXM.
This interaction may be exacerbated by apparently lower NMDAR levels in older patients.
The patient was also on the dopaminergic antagonist metoclopramine, which is metabolized by CYP2D6 and could have an additive effect on sedation. Methadone may raise the concentration of several drugs metabolized by CYP2D6.
COI: Not reported
(Achamallah, 1992) – Visual hallucinations from the combination of DXM and fluoxetine
32-year-old female with a 20-year history of dysthymia. She presented with major depression symptoms. Fluoxetine 20 mg/d was started.
On the 17th day of fluoxetine, she had cold symptoms and took two teaspoonfuls of cough syrup containing DXM. She had no prior side effects with DXM.
The next morning she took two teaspoonfuls with her fluoxetine dose and two hours later began reporting vivid hallucinations of bright colors and distortions of the shapes and dimensions of her surroundings. The hallucinations lasted 6-8 hours. They were very similar to her past experience with LSD 12 years earlier.
She then stopped fluoxetine and antidepressant treatment generally, without recurrence of visual symptoms.
COI: Not reported
(Rivers, 1970) – Lethal reaction from DXM and phenelzine
26-year-old female. She was on phenelzine 15 mg four times daily for depression. She then used approximately two ounces of a DXM cough preparation.
30 min after ingestion
Nausea and dizziness. Then she collapsed and was brought to the hospital within an hour.
Arrival at hospital
Unconscious with rigid extremities and fixed dilated pupils. She was severely hypotensive and her systolic pressure did not rise about 70.
Her temperature varied from 42 to 42.2°C. She was given various drugs including aramine, levophed, inderal, xylocaine, and adrenaline, but without effect.
4 hours and 15 min after arrival: She died from cardiac arrest.
The pathologist’s opinion was that the hyperpyrexia was of a degree and duration that was likely to be lethal itself and more likely to be so in combination with cerebral hypoxia.
COI: Not reported
Animal Studies
(Sinclair, 1973) – It produces significant toxicity and death in rabbits when combined with MAOIs
Rabbits were treated with phenelzine, pargyline, or nialamide on 2 successive days. DXM (5 mg/kg) was then given IV.
The experiments were also repeated with the pretreatments: chlorpromazine or cyproheptadine; PCPA; 5-HTP; or α-methyl-p-tyrosine.
Results
DXM (5 mg/kg) produced motor restlessness, shivering-like tremors, hyperexcitability, dilated pupils, tachypnea, and hyperpyrexia in phenelzine-treated rabbits. 5/7 rabbits died within 1 hour of DXM.
The same dose of DXM in animals not given an MAOI produced none of the symptoms or fatalities.
A lower 3 mg/kg dose of DXM produed similar but generally less intense symptoms when combined with phenelzine. 1/4 rabbits died.
DXM caused reactions with other MAOIs as well. The interaction was somewhat less intense after pargyline (2/7 died), whereas it was intense with nialamide, with all four animals dying.
This interaction was fully blocked by preadministration of chlorpromazine and partially blocked by cyproheptadine. All four chlorpromazine animals survived, while 3/4 survived with cyproheptadine.
Pretreatment with the tryptophan hydroxylase inhibitor, PCPA, also prevented the interaction. While the tyrosine hydroxylase inhibitor, α-methyl-p-tyrosine, was ineffective.
Pretreatment with 5-HTP produced similar symptoms to the MAOI-DXM interaction, indicating serotonin involvement in the interaction.
COI: Work was supported by the Medical Research Council of Canada.
Neurological Problems
There has long been a concern about NMDAR antagonists causing neurotoxicity. Although neuronal vacuolation in the form of “Olney’s lesions” does not seem to be a concern even in rodents unlike what’s seen with other NMDAR antagonists (Carliss, 2007), other forms of neurotoxicity could exist, especially with chronic use.
A high dose of DXM was found to produce myelinoid bodies and mitochondrial dysfunction in rats (Tran, 2016).
Memory impairment is a known issue with DXM, at least acutely. Animal research has found exposure to 40 mg/kg IP in rats for a week early in life can impair memory performance and alter NMDAR expression 18 months later (Zhang, 2007).
(Tran, 2016) – A high dose of DXM in rats can produce myelinoid bodies and mitochondrial dysfunction in hippocampus
Since DXM binding sites are mainly located in the CA1 region of the hippocampus, that was the area of focus in this study.
DXM was administered at 80 mg/kg IP to rats. The rats were killed one day later.
Results
It resulted in mitochondrial dysfunction and formation of myelinoid bodies in the hippocampus. There were irregularities and swelling in the crista of hippocampal mitochondria.
DXM produced malondialdehyde (marker of oxidative stress) and ROS in the cytosolic and mitochondrial fraction of rat hippocampus.
MK-801, an NMDAR antagonist, attenuated DXM-induced cytosolic oxidative burdens. However, neither MK-801 nor naloxone affected mitochondrial dysfunction from DXM and formation of myelinoid bodies.
Doses of DXM under 80 mg/kg IP failed to produce ultrastructural neurodegenerative changes. Also, a major metabolite, DXO, failed to produce the same negative effects at 80 mg/kg.
SC and orally administered doses did not lead to the same myelinoid bodies. Prior reports have shown maximal levels of DXM is higher IP vs. SC.
(Zhang, 2007) – DXM in adolescence can impair learning performance later in life for rats
Rats received DXM during postnatal days 28-37 at 40 mg/kg (IP). Rats then remained in the facility undisturbed for testing at 18 months.
Results
All rats showed a progressive decline in the escape latency regardless of treatment during the initial 9 consecutive training days, which included four trials each day.
During a Day 10 probe test (first trial of the tenth day w/ escape platform removed) memory retention was tested.
In males, there was a significant effect in males, but not females. DXM-experienced males spent less time in the target quadrant where the escape platform used to be placed vs. control males.
Reversal training (Days 12-15; assess rats’ ability to learn a new escape platform location, with the platform placed in an opposite location from the earlier trials on Days 9-10, last three trials of Day 10, and four trials on Day 11)
Females performed significantly worse on the second trial day. Swim paths of the female DXM group in the water waze task appeared to be greatly extended.
Testing did not indicate that this lower performance was the result of deficits in physical performance.
NMDAR1 expression significantly increased in the hippocampus, but not the PFC, of DXM-experienced male rats by 18-20 months of age.
While for females, increased in expression by DXM were found in both the PFC and hippocampus, suggesting repeat DXM administrations in adolescence can permanently increase NMDAR1 expression in those brain regions.
Plasma corticosterone
Basal levels of corticosterone were significantly increased in female, but not male, DXM group rats.
But when exposed to a cold stress, DXM group rats did not have a significant rise in corticosterone, unlike the placebo rats, indicating a blunting of the response to the HPA axis.
COI: Not reported
(Carliss, 2007) – DXM is not associated with neuronal vacuolation in rats
Background
Several NMDA antagonists, including MK-801 and ketamine, are associated with lesions in the brain. The lesion, sometimes known as Olney’s lesions, involves neuronal vacuolation in the retrosplenial/posterior cingulated cortices (RS/PC).
A low single dose can produce reversible vacuolation limited to the RS/PC. It’s evident 4-8 hours after dosing but is gone by 24 hours. And these changes are also not sustained with repeated dosing (up to 4 days) with MK-801, indicating rapid development of cellular tolerance.
At higher doses, however, irreversible neuronal necrosis occurs with associated reactive gliosis and disseminated changes involving additional corticolimbic structures.
Rats were exposed to DXM in single and repeat-dosing paradigms.
The single-dose study involved female rats receiving 120 mg/kg (oral)
For the repeat-dosing, the first study exposed rats to 0, 5, 25, 50, or 90 mg/kg per day for 30 days. Since no vacuolation or degeneration was seen, the dose was increased for a second study.
The second study involved 30 days of 150, 275, or 400 mg/kg for males and 120 mg/kg per day for females (females are more susceptible to damage and to mortality from DXM). There were 24 rats per sex.
Results
No DXM-related deaths or adverse behavioral effects were seen with the single or first repeat-dosing study. In the second study, four deaths occurred in males receiving 400 mg/kg and one death occurred in the female rats receiving 120 mg/kg.
MK-801 (positive control with single 9 mg/kg oral)
MK-801 led to the characteristic microscopic changes in the RS/PC confirming the methods used in these studies were appropriate to detect lesions. All animals had cytoplasmic vacuolation in the RS/PC cortex at 4-6 hours after dosing. The vacuolation was no longer seen at 48-52 hours, but there was distinct argyrophilia in the RS/PC cortex of all treated animals. Neuronal argyrophilia was also found in the piriform cortex, the indusium griseum, the dentate gyrus of the hippocampal formation, midbrain, pons, and medulla.
Necrotic neurons, based on H&E stained sections, were shrunken and angular and had brightly eosinophilic cytoplasm and dense angular nuclei.
Female rats receiving a single DXM dose and female rats given 5-400 mg/kg did not have any detectable microscopic lesions. The cytoplasm of these animals was comparable in cellular organization and overall integrity to neurons given vehicle alone.
COI: Studies were paid for by Endo Pharmaceuticals and the authors are employees of Endo Pharmaceuticals.
Dependence
Some people do become psychologically dependent on DXM and the literature indicates heavy chronic use tends to produce psychological problems (e.g. mania, delusions) and a reduced need for sleep. It’s very common to see frequent users report sleeping just 2-4 hours per night, while feeling energized during the day. This lack of proper sleep conceivably contributes to the psychological problems commonly seen with daily or near-daily use.
Mood problems and fatigue may occur when use stops, but DXM does not have a well-characterized or prominent withdrawal syndrome.
Tolerance does build over time, forcing people to use higher doses to obtain the same effects.
(Martinak, 2017) – Case report of addiction and psychosis
40-year-old female. First took it at age 29; stated she “loved it from the first try” and felt it “brought me closer to God.” The drug’s accessibility, low cost, and lack of detection on urine drug screens were relevant factors. Typical daily dose of 1080 – 1620 mg.
For five years she was taking it 3-4 times per month. This increased due to psychological stress, leading to daily abuse along with cannabis and alcohol for ~6 months, while averaging 3 hours of sleep.
Binged multiple times with 3000 – 4000 mg, leading to periods of amnesia and car accidents.
One instance led to a psychotic episode in which she thought her mother was trying to kill her so, so she planned to stab her mother and was subsequently arrested and put in a rehab.
Admitted after being found sleeping in a stranger’s house and she also assaulted a police officer.
Mirtazapine was started but most symptoms remained. Olanzapine then helped.
COI: None
(Roy, 2015) – Dependence with episodes of psychosis. Resolution of craving with topiramate.
45-year-old female. History of opioid dependence, depression, and OCD. She presented to a rehab center secondary to DXM dependence.
She was first introduced to cough syrup after having “walking pneumonia” 8 years earlier. She vividly recalled the euphoria and stimulation from it. This led to taking DXM immediate release at 120 to 180 mg/d continuously, except for during periods of jail or probation.
She also committed theft to maintain her DXM habit, which reached 800 mg per dose, sometimes multiple times per day, due to tolerance.
She had intense cravings for DXM during her imprisonment.
Withdrawal: Severe fatigue, depression, and a sense of restlessness.
Intense craving was the main driver of her inability to reduce use. She often took greater dosages than intended.
Multiple psychotic episodes occurred in connection with the use. Admitted to the ED at least 4 times for that reason. She had auditory and visual hallucinations accompanied by tachycardia, diaphoresis, hyperventilation, and a sense of doom.
She recalled having “brain burning” then she tried to “cut addiction out” by repeatedly stabbing herself with scissors, resulting in psychiatric admission. Yet, despite this, she continued using DXM.
In the rehab center her condition was observed in a state of withdrawal. After the persistence of debilitating cravings for 8 days she began receiving topiramate based on its common NMDAR action. She had full resolution of craving in 4 to 5 days. She also reported decreased craving for sugar.
Patient was then found to be homozygous (C:C) at rs1065852, indicating normal CYP2D6 function. And homozygous (C:C) at rs2832407, the GRIK1 gene.
(Linn, 2014) – Case of dependence, but no withdrawal upon cessation.
30-year-old male. He had a history of oxycodone and ethanol abuse, but he had been abstinent from those for ten months. He was using large doses of DXM, around 1440 to 1800 mg per day for 6 years.
He had been repeatedly treated for DXM dependence. He reported the drug gave him “dumb and numb” feelings so he would not “have to think [about] his problems.”
He reported marked fatigue and depression on days he did not ingest it.
On the current admission for detox his DXM urine level was 2000 ng/ml.
His physical exam and labs were normal. Liver function was normal.
Upon stopping the latest time he did not have any withdrawal symptoms.
COI: Funding came entirely from the author’s department.
(Akerman, 2010) – Case report of abuse and physical dependence signs
17-year-old male. Daily use of DXM in the form of Coricidin HBP Cough and Cold. Use increased over time from 480-960 mg/d to 1440-3840 mg/d over a period of months.
That use was continued for over a year. It was obtained from pharmacies and from websites.
Described the high as lasting 3 hours and including a sense of well-being, calmness, weightlessness, and a “greater understanding of life.”
He also said it improved his concentration and focus; he was diagnosed with ADHD.
Dependency signs appeared over time. Stopping use yielded sweating, weakness, nausea, insomnia, tachycardia, anxiety, and cravings.
Admission to treatment facility. 1.5 days before admission: Took 80 tabs of Coricidin (2400 mg) at once.
At admission, he was hypertensive, tachycardic, diaphoretic, and flushed. Craving was experienced.
Treatment with clonidine resolved the vital sign abnormalities.
During the first month of abstinence, he had dysphoria, passive suicidal ideation, anhedonia, and insomnia. Symptoms then spontaneously resolved.
COI: None
(Mutschler, 2010) – Case of dependence and addiction. Minimal withdrawal symptoms.
44-year-old male presented for addiction treatment and detox. He was taking up to 1800 mg/d of DXM tablets. He presented for treatment due to an increasing reduction in his general ability to function, which had brought on problems at work.
He had been spending over 300 euros monthly on the drug and had been dependent on the substance for about 5 years.
He noticed physical withdrawal symptoms when attempting to cease consumption since about 1 year before admission.
Initially he liked the drug because it provided a pleasurable sedative and intoxicating alcohol-like effect, but that disappeared over time.
Withdrawal symptoms reported by patient: sleep disturbance, nausea, and hyperhidrosis.
Presentation at admission
Alert, lucid, and well-oriented. Pleasant and cooperative. Concentration and attention were slightly reduced but there was no marked memory impairment. No delusions or hallucinations. Formal thinking was slowed with some prolonged delays in responding.
Mood was slightly depressed and there was some loss of affect. Drive was diminished. Psychomotor tests were normal.
No anxieties or compulsions. Appetite and sleep were undisturbed. There was no indication he was a danger to himself or others.
Medical and neurological exam were normal except for slight ataxia towards the end of the first finger-nose test. ECG was normal.
Urine at admission was positive for DXM. Follow-ups during the inpatient stay were negative.
Withdrawal symptoms (as per Clinical Institute Withdrawal Assessment)
During first 2 days: Highest score was an 8 out of 67
First day abnormalities were raised BP at a peak of 160/90 and raised HR up to 108, along with a tendency to sweat. These returned to normal on the 2nd day.
No medical treatment was needed for the autonomic withdrawal syndrome.
COI: None
(Desai, 2006) – Case of chronic addiction to DXM cough syrup with some withdrawal symptoms
66-year-old female with a history of alcohol addiction. She presented to the hospital with a complaint of “trembling” she attributed to her chronic, excessive use of DXM-containing cough syrups and she believed she was going through withdrawal.
She had a 30-year history of heavy alcohol abuse.
After quitting alcohol she eventually found DXM gave her euphoria similar to that of alcohol and could distract her from her personal problems. She then began consuming up to 4 oz of cough syrup occasionally, leading to a “high” and sometimes lethargy.
She usually took CVS brand syrup with 10 mg DXM and 100 mg guaifenesin per 5 mL.
She came to need higher doses, leading to 8 oz/day then 16 oz/day, meaning she was taking approximately 960 mg of DXM each day.
On presentation she reported taking her last dose 3 days prior. She complained of abdominal pain, nausea, and one episode of vomiting. She also complained of tremors in both hands, along with feeling depressed, dysphoric, and having insomnia.
Physical exam: Alert, cooperative, and in no acute distress. BP 183/91, HR 96, temperature 99°F, and respirations 16. She had mild coarse tremor of her outstretched hands and mild rhonchi throughout both lung fields.
She was given low-dose chlordiazepoxide (oral) for symptoms of “trembliness.” Then she was discharged 2 days later with a treatment center referral.
COI: Not reported
(Miller, 2005) – Case of psychosis, dependence, and physical withdrawal symptoms
38-year-old female. First took DXM at 33. She was taking it fight a cold and was drinking OTC Tussin DM. She reported the drug offered an energy boost, leading to her consuming 3 ounces on two separate occasions and finding she became more sociable.
Within 6 months of first taking it, she switched to daily use and then several times per day. She was developing tolerance.
At her peak of regular use she took 24 ounces per day. Her single highest daily use was roughly 40 ounces of syrup, or 2400-3600 mg DXM.
Effects lasted 3-4 hours during which she had paranoia and delusional beliefs about being able to communicate with aliens. A separate intoxication instance involved being fully convinced her intestines had become loose, triggering profound anxiety. She also had visual hallucinations of flowers. And she experienced a tactile hallucination of “fibre” rolling around under her skin, which she interpreted as “evil” and needing to be removed, though she took no action.
She repeatedly tried to change her use to cut down on the psychotic symptoms and to primarily receive euphoria, occasional profound empathy, and social relaxation. Her longest abstinent period during this time was 7 weeks.
She had a preference order for types of DXM product:
Robitussin with guaifenesin – More pleasant w/ lower amount of psychosis
Robitussin Gel Tabs
Regular DXM syrup
DXM powder purchased online – Too powerful; intense psychosis
She continued using the drug despite negative consequences: Insomnia, weight gain, constipation, acne, frightening psychoses, losing her wedding ring, feeling like she was going to die.
Intense withdrawal syndrome that was subjectively worse during the first 3 days of abstinence
Severe intermittent vomiting, intermittent night sweats for 3 weeks, muscle aches, diarrhea for 5 days, restlessness, early insomnia, feeling cold and anxiety. No rhinorrhea, lacrimation, joint aches, tremors, gooseflesh, yawning, or psychomotor agitation.
No personal or family psychiatric history of psychoses. Intoxication symptoms reliably resolved spontaneously within hours of abstinence and only returned when she went back to using.
COI: Not reported
(Fleming, 1986) – Case of dependence with craving, but no withdrawal symptoms
30-year-old male. He was admitted to a drug dependency unit after using a white powder (believed to be amphetamine) regularly for 2-3 months. He bought the drug in London.
He was snorting it and after about 15 min would get “high,” “out of my head,” and feel “on top of the world.” He would become restless and could not sit still. The effect lasted up to 2 hours, after which he would be depressed, tired, and sometimes dizzy and nauseated.
He took the powder 2-3x daily, no more than 250 mg each dose.
Evaluation: Unremarkable mental state and no abnormalities with the physical exam. He had no particular withdrawal symptoms but complained of a continued craving for the drug.
Analysis of the powder revealed it was actually pure DXM HBr.
Co-ingredients in OTC products
It is safest to take products that only contain DXM. A large portion of OTC products contain an analgesic (e.g. paracetamol, aspirin), a decongestant (e.g. phenylephrine, pseudoephedrine), an antihistamine (e.g. chlorpheniramine, brompheniramine, pheniramine), and/or the expectorant guaifenesin.
Some of the combinations, such as products containing guaifenesin, typically just lead to GI problems. Whereas combining it with paracetamol/acetaminophen can be very dangerous at recreational doses. Even guaifenesin can occasionally cause significant health problems, such as renal failure (Small, 2014).
(Small, 2014) – Renal failure attributed to guaifenesin in a DXM product
22-year-old male presented to the ED with flank pain and hematuria. The pain started several hours prior and was associated with dysuria, decreased urination, and hematuria.
The patient said he had used 10 tablets of Mucinex DM a day before the onset of symptoms. The ingestion was recreational in nature with the goal of “getting high.”
It was either 6000 mg guaifenesin and 300 mg DXM (normal strength) or 12000 guaifenesin and 600 mg DXM (max strength)
He was afebrile, had a HR of 90, and a BP of 150/78 in the community ED. Serum creatinine was elevated to 1.52 mg/dL. CT scan showed evidence of bilateral obstructing ureteral stones.
Given 1.5 mg lorazepam, 4 mg morphine, and a bolus of normal saline.
Arrival at referral facility: 98.1°F, HR 85, and BP fluctuating between 146/62 and 206/99. Tachypneic with respiration of 20.
Serum creatinine was 2.5 mg/dL, indicating progressive kidney injury. White blood cell count elevated to 21.1E9 cells/L. Urine was grossly bloody in appearance.
Serum sample negative for paracetamol and salicylates.
Given 4 mg IV ondansetron and saline.
Debris from the ureteral and bladder aspirates were sent for lab analysis and found to contain primarily guaifenesin metabolites.
Discussion
Guaifenesin nephrolithiasis was first reported in 1999. Most of the patients at that time were taking nonprescription combined preparations of guaifenesin and ephedrine chronically. A guaifenesin metabolite, β-2-metoxyphenoxy-lactic acid was identified as the main stone component.
It’s been estimated 35% of urinary stones related to pharmaceutical metabolites are related to guaifenesin.
COI: Not reported
Overdose/Problematic Effect Reports
High doses have caused acute psychosis, mania, aggressive behavior, and dangerous behavior. Some of the cases involve worsening or triggering of underlying psychiatric problems, while others involve people who were otherwise seemingly healthy.
(Gibaja, 2016) – Review of reports to a French toxicovigilance system
Analysis of all reports of DXM-related cases reported to the French Toxicovigilance and Poison Control Centers (CAPTV) system. This retrospective study looked at data from January 1999 to December 2014.
Results
1474 total cases involving DXM. 478 were associated with symptoms and there were 14 serious cases.
The number of exposures and symptomatic cases gradually rose during the study period, especially post-2007.
Among the 478 symptomatic cases, 196 were an intentional use of DXM-containing formulations: 67 addictive behaviors, 63 misuses, 66 suicide attempts
135 of the other 196 intentional exposure cases involved only DXM use with no other drugs.
Doses of DXM were similar for suicide attempts and addictive behavior cases (mean of 500 vs 375 mg), while they were lower than cases of misuses, which had a mean of 200 mg.
COI: None
(Stanciu, 2015) – Case of mania following a supratherapeutic dose
20-year-old female with no psychiatric history was brought to the ED by police due to being found outsider her apartment displaying “bizarre behavior.” She had been screaming in public, was agitated with rapid speech, had delusional disorganization, and had grandiosity. She reported auditory hallucinations consisting of communications with God.
She was combative at the ED and a psychiatrist found her to be guarded with pronounced mood lability. She had pressured speech, panic anxiety with paranoid and goal-directed content. She was paranoid about her roommates being jealous of her and wanting to rob her.
Admitted and received risperidone 1 mg twice daily, with agitation being controlled with lorazepam 1 mg.
Identified cotinine, DXM, chlorpheniramine, and DXO. Quantitative testing showed DXM at a level of 49 ng/mL.
Second hospital day: Paranoid ideas and emotional lability. By the third day she was dramatically improved in a calm state: agitation-free, paranoid ideation-free, and hallucination-free.
Acknowledged using Coricidin (DXM 30 mg; chlorpheniramine 4 mg) tablets for the first time and having done so at five times the recommended dose.
Reported increased energy after use and a decreased need for sleep.
The day before discharge she was euthymic and free of all symptoms.
COI: Not reported
(Witter, 2015) – Triggering of bipolar symptoms from underlying disorder by DXM
16-year-old male. He had an unmasking of bipolar disorder with DXM abuse and overdose. He was admitted following bizarre behavior (including an act of running down the street waving a stick) and lack of sleep for 3 nights.
3 days pre-admission
Took 20x OTC pills containing 30 mg DXM each (600 mg total)
And he had been taking about 300 mg per week for a month before admission, then increasing to 600 mg per use per week in the two weeks before hospitalization.
He said the drug had opened his mind.
Exam: Euphoria, grandiosity, delusional thinking, distractibility, psychomotor agitation, flight of ideas, and pressured speech.
He was medically stable and his lab tests were within normal limits.
Treatment: risperidone. The dose was increased over the course of treatment. And he received lorazepam for acute agitation and sleep.
Within the first 3 days of treatment minimal improvement was seen. He had elevated mood, increased energy, grandiosity, impulsivity, distractibility, and delusional thinking.
Condition gradually improved over the next 3 days and he was deemed safe for discharge (with a risperidone prescription) by Day 8.
The lack of resolution until 10 days after DXM ingestion, along with the history of possible hypomanic episodes, was consistent with a diagnosis of primary bipolar disorder.
5 months post-discharge: Stable on risperidone. Some depressive symptoms.
COI: Not reported
(Aytha, 2013) – Case of acute psychosis
40-year-old male. Hospitalized in the ICU for acute psychosis and irritable mood. Brought in after being found at a supermarket exhibiting bizarre behavior. He had purchased and rapidly ingested around 30 tablets of Coricidin HBP (each tablet had 30 mg DXM and 4 mg chlorpheniramine). Estimated dose = 900 mg DXM.
Presented tremulous and diaphoretic. Clouded sensorium, euphoric mood, and circumstantial thought process. Believed he could “look at people and know exactly what they were thinking.” He also had paranoid behavior.
He’d been abusing Coricidin HBP “to get high” for the past several weeks.
Treated with IV lorazepam; gradually discontinued over a 2-day period. Eventually he showed full remission without any need for antipsychotic treatment within 2 days after discontinuing Coricidin HBP.
COI: Not reported
(Modi, 2013) – Suicidal and homicidal behavior associated with DXM abuse
46-year-old female. She was brought to the hospital by police after stabbing her aunt repeatedly in the head and then cutting her own wrists in a suicide attempt. She reported feeling very paranoid, suffering from insomnia, and hearing voices “from Jesus” for the last few days.
“Jesus commanded and told me to stab my aunt along with myself so we could go to Heaven.”
Her only psychiatric history involved an unknown mood disorder, remote history of limited methamphetamine abuse 10 years prior, and excessive oxycodone use in the past 7 years following a car accident.
When she ran out of oxycodone she turned to DXM to help with opioid withdrawal symptoms due to learning of that use online.
She admitted to taking 3-4x 8-ounce bottles containing 10 mg DXM and 100 mg guaifenesin per dose.
Exam
BP 134/82, HR 133, respiration 16, and temperature 98.0°F.
Her urine drug screen and other initial lab and radiological workup were unremarkable.
Because she was restless, anxious, irritable, and having paranoid and hyperreligious delusions, along with poor insight and judgment, she received olanzapine 15 mg (IM) and then risperidone 1 mg (oral) twice daily for one day.
She was observed for 24 hours and then discharged to police custody. Upon discharge she was calm, cooperative, and denied any auditory or visual hallucinations or delusional beliefs. Her insight and judgment had significantly improved. She regretted the crime she committed.
COI: Not reported
(Logan, 2012) – Associated with assault, murder, and suicide in 5 cases
Case 1
31-year-old male (subject A) who was heavily immersed in DXM drug culture. He and his girlfriend (subject B) used the drug significantly. They also met two other people, a male (subject C) and female (subject D) who decided to relocate to live with Subject A and Subject B.
They all had intensive DXM use over a period of 12 months. They would usually ingest pure DXM purchased online at 600-900 mg then they supplemented this with OTC DXM products.
Eventually Subject D became less interested and moved out, fearing for her life due to the unpredictable behavior of A and B during their intoxication periods.
Incident
Subjects A, B, and C took the drug (C claims they took around 950 mg DXM) and watched videos of The Matrix and The Matrix Reloaded. Subject A started hitting his head on the floor, yelling “let me through,” punching holes in the drywall, and hitting his head on the wall.
Subject A was agitated and said “they’re in the walls” or “I’ve got to get them out,” which alluded to the movie. B and C tried to calm A, but he became withdrawn and nonresponsive.
A then moved to the kitchen, picked up a kitchen knife, and began cutting himself on the arms and chest. B followed him, A hugged her then drove the blade into her neck/shoulder, then stabbed himself in the chest.
C called the paramedics. A was found dead and B seriously wounded, though she did recover.
Toxicology
A (postmortem; peripheral): 4740 μg/L
C (living; whole blood): 300 μg/L
A, in the months prior, said he was “fighting his internal demons” and talking with “universe governing entities” under the influence of DXM.
Case 2
18-year-old male. He and his roommate and another friend ingested large doses of DXM (Coricidin brand) and smoked cannabis. Each subject used around a “full box” of Coricidin each. They had all used the drug prior without psychosis.
During the intoxication he thought he could fly and tried to exit through the window on the 5th floor. He was restrained by his friends but he resisted their efforts to calm them. Eventually one of them sat on his chest.
One of the friends then noticed he was not breathing and called EMS. The male was pronounced dead at the scene.
Toxciology
DXM: 1050 μg/L
Chlorpheniramine: 170 μg/L
Carboxy-THC: 25 μg/L
Case 3
15-year-old male. Drug history included using DXM in conjunction with chlorpheniramine, LSD, and cannabis.
He took 22 Coricidin pills and planned to smoke cannabis, according to friends who spoke to him as he was skipping school.
His sister saw him in the afternoon and reported he was acting “dumb, strange, and spacey” and staring at the wall.
Once his sister got home about 5 hours later he was found hanging by the neck from the closet doorknob. A nearby garbage can contained 6 empty 8-pill Coricidin Cough and Cold packs.
Toxicology
Pseudoephedrine: 170 μg/L
Chlorpheniramine: 210 μg/L
DXM: 2420 μg/L
Sertraline: under 50 μg/L
The deceased had discussed suicide and “being with his father” (who committed suicide) previously.
Case 4
13-year-old male who had used Coricidin on 3 occasions during the last week of his life. His death occurred shortly after the death of the subject in Case 3, who lived nearby; they knew each other.
He got home after being with friends and stayed in his room most of the evening. He denied using Coricidin when talking with his sister. Later two suicide notes were found, one noting he was bored and wanted something new and different, while the other indicated he took 164 pills.
Two empty 8-count blister packs were found in his room.
Toxicology (peripheral blood)
Chlorpheniramine: 2600 μg/L
DXM: 19,500 μg/L
Death was listed as chlorpheniramine and DXM intoxication; suicide.
Case 5
29-year-old male. Distant past history of opioid dependence; no other prior psychiatric history. He was high functioning, had a fiance, and had a 2-year-old child.
Several months before presentation he started taking OTC cold medications containing DXM. He shifted from weekend use to daily use, with an estimated typical dose of 300-500 mg.
His family then noticed a dramatic change in behavior and he became easily agitated, socially withdrawn, and had quick/pressured speech. He claimed he could predict the impending crash of the stock market and heard voices that’d give him info about the government.
He became physically aggressive in an altercation with the police, who had to be called due to his family becoming alarmed then confronting him.
After 2 days of symptomatic treatment in the hospital his behavior returned to baseline and there was no recurrence.
(Majilesi, 2011) – DXM abuse leading to seizures or seizure-like response
19-year-old female brought to the ED due to “shaking” that was noticed by witnesses. She did not remember the events. History of bipolar disorder and current medications included minocycline and lamotrigine, along with a recent initiation of aripiprazole.
Vitals and exam were unremarkable. CT and ECG were normal. Diagnosed with new-onset seizure and discharged for outpatient workup.
2 months later – Brought to ED again with a similar presentation. She was normal at work in the morning but then developed tonic-clonic movements and a period of confusion. She had no memory of the events.
Clinical exam was significant for horizontal nystagmus and tachycardia at 110.
Alert and conversant, but had a flat affect. Second CT scan of the head was normal. EEG was only remarkable for sinus tachycardia.
Admitted to abusing DXM for the past several months.
Toxicology
Serum DXM – 988.3 ng/mL
COI: Not reported
(Amaladoss, 2011) – Psychosis attributed to DXM use
20-year-old female. Brought to the hospital by police after making multiple complaints to 911. She described having bizarre somatic delusions and stated a medical doctor had injected “Salium” into her anus until it shocked her.
She was paranoid and mentioned “someone was draining her bank account.” She also described having blackouts and imagining things.
She had an increasing sore throat for 3 weeks and reported using frequent amounts of cough syrup to relieve her throat and to aid sleep. She reported taking “frequent tablespoons of cough syrup a day.”
Her only medications were trazodone 50 mg oral and temazepam 50 mg oral as needed for sleep; she also received morphine and ketorolac in the ED for pain associated with sore throat during visits to the ED in recent days for her condition; she also received clindamycin recently for the sore throat as well.
Admission: BP 106/67, HR 74, respirations 16, and temperature 36.2°C
Urine tox screen: positive for opioids, paracetamol, benzodiazepines, and TCAs
Exam: Talkative with pressured speech. She described her mood as “good,” and her affect was labile. She had delusional thoughts of the somatic and paranoid type. Her thought process was circumstantial, with occasional tangentiality. She had dissociative perceptual changes but she was not delirious. Cognitively she was awake and alert. She was admitted with the provisional diagnosis of substance-induced psychosis.
Over a 4 day hospital period she improved with olanzapine and her manic symptoms and psychosis disappeared entirely, allowing for discharge. She has been stable since with no episodes of mania or psychosis.
COI: None
(Jamison, 2009) – Agitation and psychosis associated with DXM alongside opioids
60-year-old female. Became agitated and psychotic after ingesting DXM and opioid analgesics. She had religious delusions, acted out violently towards paramedics, and had visual hallucinations. Was amnestic for a car trip that ended in a collision. Olfactory hallucinations like a strange smell in her apartment.
Medication history included propoxyphene and hydrocodone-acetaminophen along with atenolol, furosemide, and esomeprazole.
She was taking more than the recommended amount of DXM for symptomatic relief of upper respiratory infection during the week before admission, hoping larger doses would give more relief.
Presented alert, agitated, and believing she had been in the ED for 4 days. Fluent but nonsensical speech.
Treated with lorazepam and olanzapine. Completed treatment for a URTI, but mental status remained unchanged. Then she gradually responded to higher amounts of olanzapine: lower delirium, agitation, and thought disorder.
It’s possible that part of this case stemmed from DXM’s CYP2D6 metabolism, which could be inhibited by propxyphene.
COI: Not reported
(Matin, 2007) – Near fatal suicide attempt in a patient with poor CYP2D6 metabolizer status
66-year-old male.
No prior psychiatric history.
Presented after attempting suicide by slashing his forearm with a knife and ingesting bleach. The patient reported trouble recalling the exact events leading to the attempt, but he had heard voices telling him to hurt himself. His next memory after the voices was waking up to his family finding him covered in blood.
He denied any depression, mania, or psychosis and appeared perplexed by his own suicide attempt. According to his family, he had odd behavior in the week prior to admission, mentioning there were spirits in his house and he was overly suspicious in general.
Medications included amoxicillin/calvulanate for URI and a cough syrup. He admitted to taking 1575 mg/d DXM initially and then he started taking it up to six times per day.
Testing then showed he was a CYP2D6 PM.
COI: Not reported
(Hendrickson, 2007) – Case of unresponsiveness and hypotension after DXM
20-year-old male was brought to the ED by his friends after he orally ingested approximately 1 gram of liquid “Crystal Dex.” He had become unresponsive and his friends manually induced vomiting.
2 hour after ingestion: arrival at ED
Obtunded, HR 99, hypotension of 70/30, and shallow respirations.
2 mg naloxone and 1 mg flumazenil, both IV, were ineffective for respiration and arousal.
After 1 L crystalloid, BP increased to 92/50. Pupils were noted to be large and sluggish. Skin was dry, cool, and flushed. Axillary sweat was present, bowel sounds were hypoactive, and mucous membranes were moist. Patient remained obtunded after intubation.
5 hours after admission
Agitated, increased psychomotor activity with tremors and myoclonic jerks, and hypertension at 202/88. Treated with midazolam and metoprolol. He continued to have tremor, 120 HR, and agitation. Those were treated with ongoing IV midazolam.
13 hours after arrival
Agitation and tachycardia resolved. He was extubated and confirmed his ingestion of liquid “Crystal Dex” which he had purified from a cold preparation containing guaifenesin and DXM using the “Agent Lemon” technique.
No toxicological confirmation
COI: Not reported
(Price, 2000) – Case of acute psychosis
18-year-old male. Presented to psychiatric ED after several days of using cough syrup (one to two 8-oz bottles of DXM cough syrup per day; each with 711 mg per bottle).
Reported dissociative phenomena, including the belief that he had died and had “become just his thoughts.” Also out of body experience. Visual hallucinations, including the ability to “see 360-degrees in all four quadrants” and to literally “see into people.” Had delusions of telepathy at school, with the ability to ascertain the thoughts of students he sat next to. He also had paranoia, believing his employer and strangers were trying to kill/hurt him.
Showed complete remission without treatment within 4 days of discontinuing DXM abuse. Discharged with no evidence of psychosis.
Rehospitalized twice over the next 2 months with similar symptoms. Both involved DXM use. And then during a sustained abstinence from DXM during outpatient substance abuse treatment, he had no recurrent psychosis.
COI: Not reported
(Polles, 1996) – Two case reports involving mania
Case 1
43-year-old attorney. Brought to the hospital by police after shouting for help while half-clothed in front of his neighbors; was wielding a gun in a frantic effort to free his wife who was allegedly being held hostage.
History of mania subsequent to abusing propoxyphene and hydrocodone.
12 weeks before admission: Taking Delsym Cough Formula for a cold and found himself energized after doses of the syrup. This led to daily use and eventually stashing bottles to hide his growing use from family and friends. Sleep diminished to 3 hours/night.
Displayed endless energy and a euphoric mood, bought original artwork, two airplanes, a Mercedes-Benz automobile, a yacht, and an offshore island over a period of weeks.
In the weeks pre-admission, he began having flights of ideas, auditory hallucinations, and a paranoid belief that he would be killed if he fell asleep.
After stopping the drug, he was detached and dreamy for the first two days. But then his mental status, including sleep/wake cycle and psychomotor state, were entirely normal by the 4th day of admission.
Case 2
28-year-old male
3 weeks pre-admission: Began taking a cough syrup with DXM and pseudoephedrine for a persistent cough. After finding the dose led to increased energy and a sense of well-being, he kept taking more. Then he was consuming 3 bottles daily during 3 weeks to maintain this brightening of mood and energy.
After several days of abusing DXM, he also returned to abusing hydrocodone, diazepam, and alcohol.
Admission: Said “I want to stay awake all the time and do something. There’s not enough hours in the day.” He described his mood as crazy and manic.
Showed racing thoughts, distractability, and restlessness. Mood was irritable and elated.
Within 48 hours of stopping, the racing thoughts, irritability, and pressured speech subsided. After becoming abstinent his symptoms of mania went away.
COI: Not reported
(Wolfe, 1995) – Case of acute confusion
23-year-old male. Found in the snow while “agitated and hallucinating.” Had an addiction to DXM and had taken 2160 mg that day, along with several drinks of alcohol.
Examination: drowsy and easily distracted. Mildly confused; oriented to name and year but not to month or location.
Skin hot and markedly diaphoretic. Horizontal and vertical nystagmus. Extremities showed marked tremulousness and hypertonicity.
Neurological exam showed marked ataxia. Had to be helped to avoid falling.
Initial treatment with charcoal, thiamine, and naloxone was ineffective.
Symptoms gradually improved over the next 3-hours; increased ability to concentrate and he gave a more reliable, complete history.
ECG showed notched T waves and prominent U waves in leads I, II, and V2-V6
Chronic symptoms
Thousands of mg of DXM per day for the last two years and frequently during the previous five years. Also had 6 beers per day.
Daily symptoms included unstable gait, restlessness, increased intensity of perceptions, blurred vision, nausea, vomiting, shivering, severe insomnia, slurred speech, tremors, “comfortably numb” sensation, floating and flying sensations, forgetfulness, visual and auditory hallucinations, and dysphoria and severe craving after drug withdrawal.
COI: Not reported
(Murray, 1993) – Two cases of problematic effects potentially stemming from recreational use in young people
Case 1
16-year-old male. Admitted due to self-destructive behavior including self-mutilation. He’d been on treatment for depression for 6 months (imipramine) but he was not taking the medication at the time of hospitalization.
Admission: Had multiple self-inflicted lacerations on arms and chest. Otherwise in good condition. Denied suicidal or violent thoughts though he admitted frequent conflicts with his parents.
Admitted to cannabis use on weekends, drinking 8-9 beers nightly, and drinking Robitussin to “get drunk.”
He reported he and friends used Robitussin as an alternative to alcohol and other drugs. He used three 8 oz bottles weekly to feel “high” and “drunk.”
Urine drug screen was positive for cannabinoids, he also had an elevated bilirubin at 1.5 mg/dL (normal: 0.1 to 0.3 mg/dL), and mild proteinuria.
Mother reports he continued to have problems including arrests and abusing recreational drugs following discharge.
Case 2
14-year-old male brought to ED in restraints after taking multiple drugs, including 4 oz Robitussin. Father noted he had a seizure-like episode during which has was unresponsive and stiff, and he was otherwise incoherent. Awake and combative by EMS arrival.
Taken to hospital and given 2 mg naloxone, gastric lavage, and charcoal.
Remained disoriented and slow to respond for 5 hours. Reported feeling better and regained his orientation. Father reported a 6-month history of experimental drug use including alcohol and amyl nitrate.
Patient had a seizure disorder that was being treated with carbamazepine. He also had long-standing behavioral problems treated by psychotherapy.
Had elevated BP at 166/93, elevated HR at 122 on admission, and urine drug screen positive for cannabinoids and carbamazepine level under 0.5 μg/mL.
(Walker, 1993) – Case of mania repeatedly occurring due to DXM abuse
History: Benylin DM was reformulated in 1990 as a single entity cough suppressant only containing DXM, which is described as lacking analgesic and addictive properties.
40-year-old male presented with a 2-week history of manic symptoms. He had been taking Benylin DM 100 ml or more regularly for about 8 years, and at times his use increased to 400 ml daily due to stress, which would invariably produce mania.
He had been admitted once for mania associated with Benylin before its reformulation (it previously also contained diphenhydramine) and then he was admitted on 3 other subsequent occasions with the reformulated version.
When given small doses of haloperidol he rapidly settled down, though he experienced craving in the hospital and this led to his continued use, again triggering mania.
(Many, 1992) – Psychiatric problems apparently from DXM use.
57-year-old male admitted voluntarily to psychiatric care unit after presenting to ER with suicidal ideation, auditory hallucinations, and a delusion that his son would commit suicide.
Ethanol, toxicology, CBC, EKG, and chemistry were normal.
History
20 years earlier he experienced suicidal ideation during a troubling time and family history revealed possible schizophrenia.
Long-term clonidine use for hypertension.
6 days pre-admission: Flu symptoms self-treated with multiple DXM products, including Delsym, Contact, and Tussin.
Delusions about his own and his son’s suicide began 2 days pre-admission.
Evening of admission: 20 min episode of irrational talking while lying in bed with glazed eyes and being non-reactive for at least 2.5 hours, followed by him saying his head was bothering him.
Exam
Clear sensorium in presence of blunted to hostile/jocular labile affect. Marked death prescient-paranoid delusions and self-referential ideation. Episodic dissociation characterized by passivity and latency in responses extended to inert, static, noncommunicative immobilization for up to several minutes.
Despite his conviction of present or impending death, he denied current intent to commit suicide or homicide.
Given haloperidol 2 mg twice daily. All other medications stopped.
Over next 2 days: rapid diminution in delusional extent and intensity and increased cooperation along with depression, dyskinesia, and rigidity.
Haloperidol stopped over the next several days.
Discharged 9 days post-admission with complete remission. Diagnosis was acute organic delusional disturbance with mood disorder secondary to OTC medication.
COI: Not reported
(Pender, 1991) – Two cases of toxicity in young patients
Case 1
3-year-old female given DXM for mild cold symptoms. Found by parents to have used a bottle, approximately 315 mg DXM. She was unsteady, barely able to stand, and walking with a staggering gait.
Exam: 99°F temp, pulse of 124, respirations 26, BP 113/68. Ataxia, wide-based gait, and lateral and vertical nystagmus
Returned to normal over a 3-hour period of observation
Case 2
11-week-old male infant. Brought in due to “stiffening and turning blue”
Parents admitted to giving him more DXM than recommended to ease cold symptoms; didn’t know the total amount given.
Exam: temp 101°F, pulse 152, respiration 38, and BP of 80.
Alert and noted to be hyperexcitable with intermittent periods of extremity stiffening and cutaneous mottling. During those episodes he was alert and appeared anxious. No postictal periods.
Except for increased tone, hyperreflexia, and irritability, neurologic exam was normal.
Within 30 min of receiving naloxone: noted to be calmer and within two hours all signs of increased tone, hyperreflexia, and hyperexcitability had resolved, as had skin mottling.
COI: Not reported
Chronic toxicity
Heavy recreational use in young people could produce a negative impact on brain development. At the least it is associated with transient cognitive impairment, a reduction in sleeping, mania, and hallucinations when it is used at high doses on a regular basis, regardless of age.
When comparing chronic DXM users to healthy controls, Qiu (2016) showed users had significantly higher attentional impulsivity, motor impulsivity, and non-plan impulsivity. They also had increased cortical thickness, and increased right thalamus and right pallidum volume. These results were taken to mean DXM could impair synaptic pruning, an important part of brain development.
(Qiu, 2016) – There is evidence of a negative impact on brain development in adolescents/young adults chronically using DXM recreationally
38 DXM-dependent individuals were studied and compared with 18 healthy controls
No significant differences in age, formal years of education, or number of cigarettes smoked per day.
DXM use for a mean of 5.15 years beginning at 18.9 years old.
Use: 481.1 ml/day
Results
DXM-dependent people had significantly higher attentional impulsivity, motor impulsivity, and non-plan impulsivity.
Increased cortical thickness in DXM abusers
Significant increases in cortical thickness in 9 clusters: 3 in the left hemisphere and 6 in the right.
The clusters were located primarily in the bilateral precuneus, left dorsal lateral PFC, left inferior parietal lobe, right lateral occipital cortex, right inferior temporal cortex, right lateral orbitofrontal cortex, right transverse temporal gyrus, and right precentral gyrus.
Increased right thalamus and right pallidum volume
The dependent individuals had significantly increased right thalamus and right pallidum volume. Other subcortical structures did not show significant differences.
Cortical thickness correlated with initial age of DXM use
Significant negative correlation between thickness in the DLPFC + right precentral gyrus and the initial age of DXM use.
Lack of significant correlation for the other clusters.
COI: None. Funded by grants from the Natural Scientific Foundation of China and the Natural Scientific Foundation of Jiangxi Province, China.
(Hinsberger, 1994) – Long-term DXM abuse associated with cognitive deterioration and psychiatric symptoms
39-year-old male. He was hospitalized in an acute manic state after his functioning had deteriorated gradually for 1 year and he had quit his job.
He had no history of any mood disorder until one year before presentation. Though he had a past history of alcohol dependence and he had abused a Diphenhydramine product previously.
During hospitalization
He was typically in a depressed state with intense suicidal ideation. He had restlessness and insomnia that was refractory to sedative-hypnotics. Though he was preoccupied with religious matters while depressed, he was rarely delusional and had no other signs of psychosis while depressed.
Sometimes he also had manic-like states with euphoria, aggressive and disruptive behavior, copious note-writing, and frequent religious experiences with communication with God and grandiose delusional ideas that he was chosen by God for a special purpose. The manic states lasted only a few days and were followed by a prolonged depressive mood.
The frequency of his mood fluctuations increased.
4 months after admission
Cognitive testing revealed a full scale IQ of 89. Other cognitive testing revealed scores that were lower than would be expected from his IQ.
He became increasingly irritable and failed to arrive for numerous appointments.
CT scan several months after admission showed nothing. A single SPECT scan showed diffuse patchy uptake in the bilateral cerebral hemispheres suggesting nonspecific widespread dysfunction.
EEG did not show seizure activity but quantitative EEG showed excessive central alpha activity, especially on the right side.
The possibility of a concurrent diagnosis of temporal lobe epilespy was considered given the episodic religiosity and hypergraphia. But he continued to deteriorate depiste an adequate trial of carbamazepine.
Manic states became more severe and suggestive of an organic confusional state, including visual hallucinations, slurred speech, ataxia, bilateral nystagmus in all directions, urinary retention, dysnomia, subjective feelings of brief severe muscle weakness and trance-like spells lasting up to 2 minutes.
Though numerous prior drug screen were negative, a more comprehensive one revealed guaifenesin and DXM.
He admitted to taking about one bottle (1500 mg DXM, 5000 mg guaifenesin, and 3.5 mg alcohol) weekly and he continued to do so for several months despite recommendation.
After ingestion he would have a manic-like state of psychosis lasting 24-48 hours followed by depression, intense suicidal ideation, and insomnia.
The cognitive deterioration persisted even in periods of abstinence for several weeks. Mood instability persisted as well and he remained hospitalized for almost another year.
He continued to abuse cough syrup whenever possible despite encouragement to refrain.
COI: Not reported
Toxicity reports in medical settings
Occasionally problems are reported in medical settings, most often in children who have received more than the recommended dose. Since most products contain other active ingredients, it’s more difficult to determine causality. Usually the effects are limited to symptoms like greater than expected drowsiness. Flushing or rash with urticaria is also fairly common.
Because of the potential for adverse effects in young children, a voluntary label change was made in 2007/2008 with FDA support. Product labels were changed to state “do not use” in children under 4-years-old, though evidence indicates DXM-containing products are still widely used in that age group.
(Paul, 2016) – Review of adverse events associated with child exposure to DXM, mainly overdose.
5342 cases in children 12 and younger were reviewed. 1716 (32/1%) reported at least one adverse event.
The cases mainly came from the NPDS, FDA Adverse Event Reporting System, and participating manufacturer safety reports.
Single-product, single-ingredient cases accounted for 773 (45.0%) of cases.
In DXM-only cases, 99.2% involved liquid preparations and 95.0% of exposures were specifically with pediatric liquid products. Notably, 93.7% were attributed to liquid extended-release DXM polisterex.
Adverse events
No deaths or pathological cardiac arrhythmias. The adverse event profile was dominated by CNS and autonomic symptoms including ataxia, drowsiness, mydriasis, tachycardia, and hallucinations, each occurring in over 20% of cases.
A generalized flushing or rash often with urticaria was seen in 18.1% of cases. Dystonia occurred in 5.4%.
Less common (3.5% of cases) events were respiratory: hypoxia, respiratory depression, apnea, decreased respiratory rate, hypopnea, hypoventilation, respiratory disorder, and respiratory failure.
Only 2.8% of cases involved a therapeutic dose. The majority where the dose were known involved supratherapeutic doses.
Children under 4 years old made up the largest group of cases with 59.6% of children.
COI: Funded by the Consumer Healthcare Products Association. Authors have also consulted for industry.
(Chu, 2016) – Mania associated with the medical use of DXM.
22-year-old female. She had a history of depression and was on escitalopram (15 mg/d) for 6 months. Then she developed an acute URTI and received 30 mg DXM every six hours.
After 4 days of DXM she had elevated mood, euphoria, psychomotor agitation with violent tendency, distraction, and decreased need for sleep. The manic symptoms impaired her functionality and she was brought to the ED.
In the ED, examination showed no notable alteration of vitals and she was oriented. Lab results and other exams were normal. She did not have a history of manic or hypomanic episodes.
She received an IM injection of lorazepam 2 mg. This produced marked sedation. After half a day, the mania resolved and did not recur in the following days. Escitalopram was continued and the episode did not recur in the absence of DXM administration.
COI: None
(Turner, 2016) – Catatonia associated with withdrawal of DXM/quinidine
65-year-old male with schizoaffective disorder and a history of pseudobulbar affect. He had been receiving 20 mg DXM plus 10 mg quinidine daily, along with lorazepam 0.5 mg four times daily. When he developed a urologic infection he was admitted to the hospital and ciprofloxacin was initiated, while DXM and lorazepam were stopped.
On Day 1 – He became stuporous. His Bush-Francis Catatonia Rating Scale was 24 and his Kanner scale, part 2, score was 64. This was consistent with severe catatonia.
The catatonia persisted over the 2-week ciprofloxacin course and for another week after it was discontinued.
He was restarted on DXM 20 mg daily but remained catatonic. Restarting lorazepam also did not resolve the symptoms. When DXM was changed to a dosing frequency of 20 mg every 12 hours, he improved and was free of catatonic symptoms within one week. He was able to return to his group home 5 weeks after admission without any catatonia at follow-up.
Discussion
Ciprofloxacin has some anti-GABAergic properties and that could have contributed to the development of catatonia, though the symptoms did not resolve alongside the discontinuation of that medication.
COI: None
(LoVecchio, 2008) – Chart review focused on accidental DXM ingestions in children under 5 years old. The effects are usually mild.
Retrospective chart review at a poison center during 2003 and 2004.
Results
110,000 charts were searched and a total of 304 cases met inclusion criteria (accidental ingestion of DXM).
Mean age of 28.2 months
All cases involved co-ingestants like paracetamol, pseudoephedrine, guaifenesin, ibuprofen, and various H1 receptor antagonists.
Approximate dose was 35.0 mg on average.
No patient had any hemodynamic instability like low BP or tachycardia that required intervention. Only 20.4% had signs of sedation.
No deaths.
Only 1 patient, a 13-month-old, was admitted after presenting with prolonged lethargy.
COI: None and no outside funding of any kind.
(Graudins, 1996) – Case of acute dystonia in a child
8-year-old male. Receiving DXM (10 mg + phenylpropanolamine and guaifenesin) every 6 hours for three days.
Day of presentation: Sleeping all day. Awoke in the afternoon with his head deviated to the right and with generalized stiffness of all muscle groups.
Arrival at ED: anxious, awake and alert, HR of 113, BP 140/80, respiration of 34, and temp 37.5°C.
Torticollis to the right, generalized extension with hypertonia of his limbs, and he was unable to speak.
Diphenhydramine 25 mg given IV, producing immediate resolution of symptoms.
Cough syrup was discontinued and there was no recurrence of symptoms.
COI: Not reported
Bromide Poisoning
Chronic ingestion of DXM HBr and/or substantial acute ingestions could hypothetically expose a user to enough bromide to cause bromide poisoning, but this has rarely been reported. Ng (1992) reported a case of a 56-year-old male who used 24 mg daily for years and then took ~75 mg on a single day, which was followed by collapse and unconsciousness. His serum bromide level was significantly elevated and hemodialysis was effective. Although the authors blamed the patient’s acute and chronic symptoms on bromide poisoning from DXM HBr, it is so rarely alleged that it’s not clear whether bromide poisoning is a true concern, even with chronic exposure.
Bromide toxicity can produce headache, weakness, apathy, skin lesions, stupor, drowsiness, and coma.
(Ng, 1992) – Case of bromide toxicity apparently caused by long-term use of DXM HBr
56-year-old male. Used 60 mL of a cough syrup product for years to combat headache. It exposed him to 500 mg paracetamol, 24 mg DXM HBr, 15 mg methylephedrine, 4.2 mg chlorpheniramine, and 75 mg caffeine per day.
Eventually he fell down on the street and lost consciousness after acutely using 3x more syrup than usual for severe headache.
Bromide intoxication was suspected, leading to hemodialysis. After 4 hours of demodialysis, his consciousness became clear.
Serum bromide fell from 2.6 to 0.65 mg/dl
Long-standing symptoms of chronic severe headache, weakness in the lower limbs, and lethargy also subsided without medication. Diagnosis of bromide toxicity could be supported by serum change in electrolytes and bromide and the improvement in clinical symptoms.
References
A Linn, K., T Long, M., & S Pagel, P. (2014). “Robo-Tripping”: Dextromethorphan Abuse and its Anesthetic Implications. Anesthesiology and Pain Medicine, 4(5). https://doi.org/10.5812/aapm.20990
Abdul Manap, R., Wright, C. E., Gregory, A., Rostami-Hodjegan, A., Meller, S. T., Kelm, G. R., … Morice, A. H. (1999). The antitussive effect of dextromethorphan in relation to CYP2D6 activity. British Journal of Clinical Pharmacology, 48(3), 382–7. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/10510150
Achamallah, N. S. (1992). Visual hallucinations after combining fluoxetine and dextromethorphan. The American Journal of Psychiatry, 149(10), 1406. https://doi.org/10.1097/gme.0b013e3181967b88
Afshar, M., Birnbaum, D., & Golden, C. (2014). Review of Dextromethorphan Administration in 18 Patients With Subacute Methotrexate Central Nervous System Toxicity. Pediatric Neurology, 50(6), 625–629. https://doi.org/10.1016/j.pediatrneurol.2014.01.048
Ahtee, L. (1975). Dextromethorphan inhibits 5-hydroxytryptamine uptake by human blood platelets and decreases 5-hydroxyindoleacetic acid content in rat brain. Journal of Pharmacy and Pharmacology, 27(3), 177–180. https://doi.org/10.1111/j.2042-7158.1975.tb09433.x
Aiyer, R., Mehta, N., Gungor, S., & Gulati, A. (2017). A Systematic Review of NMDA Receptor Antagonists for Treatment of Neuropathic Pain in Clinical Practice. The Clinical Journal of Pain, 1. https://doi.org/10.1097/AJP.0000000000000547
Akerman, S. C., Hammel, J. L., & Brunette, M. F. (2010). Dextromethorphan Abuse and Dependence in Adolescents. Journal of Dual Diagnosis, 6(3–4), 266–278. https://doi.org/10.1080/15504263.2010.537515
Al-Jenoobi, F., Al-Thukair, A., Abbas, F., Ansari, M., Alkharfy, K., Al-Mohizea, A., … Jamil, S. (2010). Effect of Black Seed on Dextromethorphan O- and N-Demethylation in Human Liver Microsomes and Healthy Human Subjects. Drug Metabolism Letters, 4(1), 51–55. https://doi.org/10.2174/187231210790980435
Allen, R. M., Granger, A. L., & Dykstra, L. A. (2002). Dextromethorphan potentiates the antinociceptive effects of morphine and the delta-opioid agonist SNC80 in squirrel monkeys. The Journal of Pharmacology and Experimental Therapeutics, 300(2), 435–41. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/11805202
Amaladoss, A., & O’Brien, S. (2011). Cough Syrup Psychosis. CJEM, 13(1), 53–56. https://doi.org/10.2310/8000.2011.100216
Askmark, H., Aquilonius, S. M., Gillberg, P. G., Liedholm, L. J., Stalberg, E., & Wuopio, R. (1993). A pilot trial of dextromethorphan in amyotrophic lateral sclerosis. Journal of Neurology, Neurosurgery & Psychiatry, 56(2), 197–200. https://doi.org/10.1136/jnnp.56.2.197
Aytha, S. K., Dannaram, S., Moorthy, S., & Sharma, A. (2013). A Case of Acute Psychosis Secondary to Coricidin Overdose. The Primary Care Companion For CNS Disorders, 15(6), 13–1549. https://doi.org/10.4088/PCC.13l01549
Baggott, M., Heifets, B., Jones, R. T., Mendelson, J., Sferios, E., & Zehnder, J. (2000). Chemical analysis of ecstasy pills. JAMA, 284(17), 2190. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/11056589
Baker, A. K., Hoffmann, V. L. H., & Meert, T. F. (2002). Dextromethorphan and ketamine potentiate the antinociceptive effects of mu- but not delta- or kappa-opioid agonists in a mouse model of acute pain. Pharmacology, Biochemistry, and Behavior, 74(1), 73–86. https://doi.org/S0091305702009619
Ballard, C., Sharp, S., & Corbett, A. (2015). Dextromethorphan and Quinidine for Treating Agitation in Patients With Alzheimer Disease Dementia. JAMA, 314(12), 1233. https://doi.org/10.1001/jama.2015.10215
Bane, A., Rojas, D., Indermaur, K., Bennett, T., & Avery, D. (1996). Adverse effects of dextromethorphan on the spatial learning of rats in the Morris water maze. European Journal of Pharmacology, 302(1–3), 7–12. https://doi.org/10.1016/0014-2999(96)00056-8
Bem, J. L., & Peck, R. (1992). Dextromethorphan. An overview of safety issues. Drug Safety, 7(3), 190–9. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/1503667
Bjoraker, K. J., Swanson, M. A., Coughlin, C. R., Christodoulou, J., Tan, E. S., Fergeson, M., … Van Hove, J. L. K. (2016). Neurodevelopmental Outcome and Treatment Efficacy of Benzoate and Dextromethorphan in Siblings with Attenuated Nonketotic Hyperglycinemia. The Journal of Pediatrics, 170, 234–239. https://doi.org/10.1016/j.jpeds.2015.12.027
Blin, O., Azulay, J. P., Desnuelle, C., Billé-Turc, F., Braguer, D., Besse, D., … Pouget, J. Y. (1996). A controlled one-year trial of dextromethorphan in amyotrophic lateral sclerosis. Clinical Neuropharmacology, 19(2), 189–92. Retrieved from http://www.embase.com/search/results?subaction=viewrecord&from=export&id=L26099377%5Cnhttp://sfx.library.uu.nl/utrecht?sid=EMBASE&issn=03625664&id=doi:&atitle=A+controlled+one-year+trial+of+dextromethorphan+in+amyotrophic+lateral+sclerosis&stitle=CLIN.+NE
Bobo, W. V, Miller, S. C., & Martin, B. D. (2005). The Abuse Liability of Dextromethorphan Among Adolescents: A Review. Journal of Child & Adolescent Substance Abuse, 14(4), 55–75. https://doi.org/10.1300/J029v14n04_04
Boland, D. M., Rein, J., Lew, E. O., & Hearn, W. L. (2003). Fatal cold medication intoxication in an infant. Journal of Analytical Toxicology, 27(7), 523–6. https://doi.org/NO_DOI
Boyer, E. W. (2004). Dextromethorphan Abuse. Pediatric Emergency Care, 20(12), 858–863. https://doi.org/10.1097/01.pec.0000148039.14588.d0
Briggs, S. A., Hall, B. J., Wells, C., Slade, S., Jaskowski, P., Morrison, M., … Levin, E. D. (2016). Dextromethorphan interactions with histaminergic and serotonergic treatments to reduce nicotine self-administration in rats. Pharmacology Biochemistry and Behavior, 142, 1–7. https://doi.org/10.1016/j.pbb.2015.12.004
Britton, P., Lu, X.-C. M., Laskosky, M. S., & Tortella, F. C. (1997). Dextromethorphan protects against cerebral injury following transient, but not permanent, focal ischemia in rats. Life Sciences, 60(20), 1729–1740. https://doi.org/10.1016/S0024-3205(97)00132-X
Bryner, J. K., Wang, U. K., Hui, J. W., Bedodo, M., MacDougall, C., & Anderson, I. B. (2006). Dextromethorphan Abuse in Adolescence. Archives of Pediatrics & Adolescent Medicine, 160(12), 1217. https://doi.org/10.1001/archpedi.160.12.1217
Carbonaro, T. M., Johnson, M. W., Hurwitz, E., & Griffiths, R. R. (2018). Double-blind comparison of the two hallucinogens psilocybin and dextromethorphan: similarities and differences in subjective experiences. Psychopharmacology, 235(2), 521–534. https://doi.org/10.1007/s00213-017-4769-4
Carliss, R. D., Radovsky, A., Chengelis, C. P., O’Neill, T. P., & Shuey, D. L. (2007). Oral administration of dextromethorphan does not produce neuronal vacuolation in the rat brain. NeuroToxicology, 28(4), 813–818. https://doi.org/10.1016/j.neuro.2007.03.009
Carlsson, K. C., Hoem, N. O., Moberg, E. R., & Mathisen, L. C. (2004). Analgesic effect of dextromethorphan in neuropathic pain. Acta Anaesthesiologica Scandinavica, 48(3), 328–336. https://doi.org/10.1111/j.0001-5172.2004.0325.x
Carpenter, C. L., Marks, S. S., Watson, D. L., & Greenberg, D. A. (1988). Dextromethorphan and dextrorphan as calcium channel antagonists. Brain Research, 439(1–2), 372–5. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/2451974
Carpenter, C. L., Marks, S. S., Watson, D. L., & Greenberg, D. A. (1988). Dextromethorphan and dextrorphan as calcium channel antagonists. Brain Research, 439(1–2), 372–5. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/2451974
Carroll, B. T. (2016). Dextromothorphan/quinidine Withdrawal Catatonia: A Case Report, (November 2015), 2015–2017.
Carter, L. P., Reissig, C. J., Johnson, M. W., Klinedinst, M. A., Griffiths, R. R., & Mintzer, M. Z. (2013). Acute cognitive effects of high doses of dextromethorphan relative to triazolam in humans. Drug and Alcohol Dependence, 128(3), 206–213. https://doi.org/10.1016/j.drugalcdep.2012.08.025
Cass, L. J., & Frederik, W. S. (1953). Evaluation of a New Antitussive Agent. New England Journal of Medicine, 249(4), 132–136. https://doi.org/10.1056/NEJM195307232490402
Chen, S.-L., Hsu, K.-Y., Huang, E. Y.-K., Lu, R.-B., & Tao, P.-L. (2011). Low doses of dextromethorphan attenuate morphine-induced rewarding via the sigma-1 receptor at ventral tegmental area in rats. Drug and Alcohol Dependence, 117(2–3), 164–169. https://doi.org/10.1016/j.drugalcdep.2011.01.013
Chen, S.-L., Huang, E. Y.-K., Chow, L.-H., & Tao, P.-L. (2005). Dextromethorphan differentially affects opioid antinociception in rats. British Journal of Pharmacology, 144(3), 400–404. https://doi.org/10.1038/sj.bjp.0706086
Chen, S.-L., Lee, S.-Y., Chang, Y., Chen, P.-S., Lee, I., Wang, T., … Lu, R. (2014). Therapeutic effects of add-on low-dose dextromethorphan plus valproic acid in bipolar disorder. European Neuropsychopharmacology, 24(11), 1753–1759. https://doi.org/10.1016/j.euroneuro.2014.09.001
Chen, S., Lee, S., Chang, Y., Chen, S.-H., Chu, C.-H., Tzeng, N.-S., … Lu, R. (2012). Inflammation in Patients with Schizophrenia: The Therapeutic Benefits of Risperidone Plus Add-On Dextromethorphan. Journal of Neuroimmune Pharmacology, 7(3), 656–664. https://doi.org/10.1007/s11481-012-9382-z
CHENG, W., LI, Y., HOU, X., BAI, B., LI, F., DING, F., … WANG, Y. (2015). Determining the neuroprotective effects of dextromethorphan in lipopolysaccharide-stimulated BV2 microglia. Molecular Medicine Reports, 11(2), 1132–1138. https://doi.org/10.3892/mmr.2014.2794
Choi, D. W. (1987). Dextrorphan and dextromethorphan attenuate glutamate neurotoxicity. Brain Research, 403(2), 333–336. https://doi.org/10.1016/0006-8993(87)90070-9
Chomchai, C., & Manaboriboon, B. (2012). Stimulant Methamphetamine and Dextromethorphan Use Among Thai Adolescents: Implications for Health of Women and Children. Journal of Medical Toxicology, 8(3), 291–294. https://doi.org/10.1007/s13181-012-0228-0
Church, J., Sawyer, D., & McLarnon, J. G. (1994). Interactions of dextromethorphan with theN-methyl-d-aspartate receptor-channel complex: single channel recordings. Brain Research, 666(2), 189–194. https://doi.org/10.1016/0006-8993(94)90771-4
Chyka, P. A., Erdman, A. R., Manoguerra, A. S., Christianson, G., Booze, L. L., Nelson, L. S., … Troutman, W. G. (2007). Dextromethorphan poisoning: An evidence-based consensus guideline for out-of-hospital management. Clinical Toxicology, 45(6), 662–677. https://doi.org/10.1080/15563650701606443
Cohen, S. P., Chang, A. S., Larkin, T., & Mao, J. (2004). The Intravenous Ketamine Test: A Predictive Response Tool for Oral Dextromethorphan Treatment in Neuropathic Pain. Anesthesia & Analgesia, 99(6), 1753–1759. https://doi.org/10.1213/01.ANE.0000136953.11583.7B
Cohen, S. P., Verdolin, M. H., Chang, A. S., Kurihara, C., Morlando, B. J., & Mao, J. (2006). The Intravenous Ketamine Test Predicts Subsequent Response to an Oral Dextromethorphan Treatment Regimen in Fibromyalgia Patients. The Journal of Pain, 7(6), 391–398. https://doi.org/10.1016/j.jpain.2005.12.010
Comi, A. M., Highet, B. H., Mehta, P., Hana Chong, T., Johnston, M. V, & Ann Wilson, M. (2006). Dextromethorphan protects male but not female mice with brain ischemia. NeuroReport, 17(12), 1319–1322. https://doi.org/10.1097/01.wnr.0000220136.98918.41
Compton, P. A., Ling, W., & Torrington, M. A. (2008). Lack of effect of chronic dextromethorphan on experimental pain tolerance in methadone-maintained patients. Addiction Biology, 13(3–4), 393–402. https://doi.org/10.1111/j.1369-1600.2008.00112.x
Cornish, J. W., Herman, B. H., Ehrman, R. N., Robbins, S. J., Childress, A. R., Bead, V., … O’Brien, C. P. (2002). A randomized, double-blind, placebo-controlled safety study of high-dose dextromethorphan in methadone-maintained male inpatients. Drug and Alcohol Dependence, 67(2), 177–83. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/12095667
Cummings, J. L., Lyketsos, C. G., Peskind, E. R., Porsteinsson, A. P., Mintzer, J. E., Scharre, D. W., … Siffert, J. (2015). Effect of Dextromethorphan-Quinidine on Agitation in Patients With Alzheimer Disease Dementia. JAMA, 314(12), 1242. https://doi.org/10.1001/jama.2015.10214
Cunningham, V. (2011). Dextromethorphan Abuse in Teens: Beware Acetaminophen Poisoning! CJEM, 13(5), 298. https://doi.org/10.2310/8000.2011.110542
Dematteis, M., Lallement, G., & Mallaret, M. (1998). Dextromethorphan and dextrorphan in rats: common antitussives–different behavioural profiles. Fundamental & Clinical Pharmacology, 12(5), 526–37. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/9794151
Desai, S., Aldea, D., Daneels, E., Soliman, M., Braksmajer, A. S., & Kopes-Kerr, C. P. (2006). Chronic Addiction to Dextromethorphan Cough Syrup: A Case Report. The Journal of the American Board of Family Medicine, 19(3), 320–323. https://doi.org/10.3122/jabfm.19.3.320
Di Marco, M. P., Edwards, D. J., Wainer, I. W., & Ducharme, M. P. (2002). The effect of grapefruit juice and seville orange juice on the pharmacokinetics of dextromethorphan: the role of gut CYP3A and P-glycoprotein. Life Sciences, 71(10), 1149–60. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/12095536
Dickerson, D. L., Schaepper, M. A., Peterson, M. D., & Ashworth, M. D. (2008). Coricidin HBP® Abuse. Journal of Addictive Diseases, 27(1), 25–32. https://doi.org/10.1300/J069v27n01_03
Donno, M., Aversa, C., Corsico, R., Foresi, A., Grassi, V., Malerba, M., … Olivieri, D. (1994). Efficacy and Safety of Moguisteine in Comparison with Dextromethorphan in Patients with Persistent Cough. Drug Investigation, 7(2), 93–100. https://doi.org/10.1007/BF03257404
Doody, R. S., D’Amico, S., Cutler, A. J., Davis, C. S., Shin, P., Ledon, F., … Siffert, J. (2016). An open-label study to assess safety, tolerability, and effectiveness of dextromethorphan/quinidine for pseudobulbar affect in dementia: PRISM II results. CNS Spectrums, 21(6), 450–459. https://doi.org/10.1017/S1092852915000620
Drachtman, R. A., Cole, P. D., Golden, C. B., James, S. J., Melnyk, S., Aisner, J., & Kamen, B. A. (2002). DEXTROMETHORPHAN IS EFFECTIVE IN THE TREATMENT OF SUBACUTE METHOTREXATE NEUROTOXICITY. Pediatric Hematology and Oncology, 19(5), 319–327. https://doi.org/10.1080/08880010290057336
Dudgeon, D. J., Bruera, E., Gagnon, B., Watanabe, S. M., Allan, S. J., Warr, D. G., … Pater, J. L. (2007). A Phase III Randomized, Double-Blind, Placebo-Controlled Study Evaluating Dextromethorphan Plus Slow-Release Morphine for Chronic Cancer Pain Relief in Terminally Ill Patients. Journal of Pain and Symptom Management, 33(4), 365–371. https://doi.org/10.1016/j.jpainsymman.2006.09.017
Duedahl, T. H., Dirks, J., Petersen, K. B., Romsing, J., Larsen, N.-E., & Dahl, J. B. (2005). Intravenous dextromethorphan to human volunteers: relationship between pharmacokinetics and anti-hyperalgesic effect. Pain, 113(3), 360–368. https://doi.org/10.1016/j.pain.2004.11.015
Duedahl, T. H., Rømsing, J., Møiniche, S., & Dahl, J. B. (2006). A qualitative systematic review of peri-operative dextromethorphan in post-operative pain. Acta Anaesthesiologica Scandinavica, 50(1), 1–13. https://doi.org/10.1111/j.1399-6576.2006.00900.x
DUHAIME, A.-C., GENNARELLI, L. M., & BOARDMAN, C. (1996). Neuroprotection by Dextromethorphan in Acute Experimental Subdural Hematoma in the Rat. Journal of Neurotrauma, 13(2), 79–84. https://doi.org/10.1089/neu.1996.13.79
Elliott, K., Hynansky, A., & Inturrisi, C. E. (1994). Dextromethorphan attenuates and reverses analgesic tolerance to morphine. Pain, 59(3), 361–368. https://doi.org/10.1016/0304-3959(94)90022-1
Elmenesy, T. M., Hamden, G. A., Abo Eldahab, H. A., & El Abd, N. A. (2011). Dextromethorphan reduced fentanyl induced cough and stress hormones release. A randomized double blind controlled study. Egyptian Journal of Anaesthesia, 27(1), 25–30. https://doi.org/10.1016/j.egja.2011.01.003
Engber, T. M., & Chase, T. N. (1988). Dextromethorphan does not protect against quinolinic acid neurotoxicity in rat striatum. Neuroscience Letters, 95(1–3), 269–74. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/2976130
Erden, B. F., Ozdemirci, S., Yildiran, G., Utkan, T., Gacar, N., & Ulak, G. (1999). Dextromethorphan attenuates ethanol withdrawal syndrome in rats. Pharmacology, Biochemistry, and Behavior, 62(3), 537–41. Retrieved from http://www.sciencedirect.com/science/article/pii/S0091305798001750
Department of Defense. (1977). Experimentation Programs conducted by the Department of Defense That Had CIA Sponsorship or Participation and That Involved the Administration to Human Subjects of Drugs Intended for Mind-control or Behavior-modification Purposes.
Falck, R., Li, L., Carlson, R., & Wang, J. (2006). The Prevalence of Dextromethorphan Abuse Among High School Students. PEDIATRICS, 118(5), 2267–2269. https://doi.org/10.1542/peds.2006-2050
Faruqi, S., Wright, C., Thompson, R., & Morice, A. H. (2014). A randomized placebo controlled trial to evaluate the effects of butamirate and dextromethorphan on capsaicin induced cough in healthy volunteers. British Journal of Clinical Pharmacology, 78(6), 1272–1280. https://doi.org/10.1111/bcp.12458
Fazli-Tabaei, S., Maghsoudi, A., Bazaz, N., Modirzadeh, A., & Zarrindast, M.-R. (2008). Effect of dextromethorphan on antinociception and tolerance induced by swim-stress in the formalin test. Archives of Iranian Medicine, 11(3), 286–92. https://doi.org/08113/AIM.0010
Feng, S., Xu, Z., Liu, W., Li, Y., Deng, Y., & Xu, B. (2014). Preventive Effects of Dextromethorphan on Methylmercury-Induced Glutamate Dyshomeostasis and Oxidative Damage in Rat Cerebral Cortex. Biological Trace Element Research, 159(1–3), 332–345. https://doi.org/10.1007/s12011-014-9977-8
Ferkany, J. W., Borosky, S. A., Clissold, D. B., & Pontecorvo, M. J. (1988). Dextromethorphan inhibits NMDA-induced convulsions. European Journal of Pharmacology, 151(1), 151–154. https://doi.org/10.1016/0014-2999(88)90707-8
Fernández-Fernández, F. J., Ameneiros-Lago, E., Lijó-Carballeda, C., & Sesma, P. (2017). Dextromethorphan and Methylxanthines Might Be Useful in the Treatment of Methotrexate-Induced Neurotoxicity. Pediatric Emergency Care, 33(5), 380. https://doi.org/10.1097/PEC.0000000000001128
Finnegan, K. T., Kerr, J. T., & Langston, J. W. (1991). Dextromethorphan protects against the neurotoxic effects ofp-chloroamphetamine in rats. Brain Research, 558(1), 109–111. https://doi.org/10.1016/0006-8993(91)90723-9
Fleming, P. M. (1986). Dependence on dextromethorphan hydrobromide. British Medical Journal (Clinical Research Ed.), 293(6547), 597. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/3092943
Ford, J. A., & Ph, D. (2009). Misuse of Over-the-Counter Cough or Cold Medications Among Adolescents : Prevalence and Correlates in a National Sample. Journal of Adolescent Health, 44(5), 505–507. https://doi.org/10.1016/j.jadohealth.2008.10.140
Forget, P., le Polain de Waroux, B., Wallemacq, P., & Gala, J.-L. (2008). Life-Threatening Dextromethorphan Intoxication Associated with Interaction with Amitriptyline in a Poor CYP2D6 Metabolizer: A Single Case Re-Exposure Study. Journal of Pain and Symptom Management, 36(1), 92–96. https://doi.org/10.1016/j.jpainsymman.2007.09.006
Forrester, M. B. (2011). Dextromethorphan Abuse in Texas, 2000–2009. Journal of Addictive Diseases, 30(3), 243–247. https://doi.org/10.1080/10550887.2011.581986
Galer, B. S., Lee, D., Ma, T., Nagle, B., & Schlagheck, T. G. (2005). MorphiDex® (morphine sulfate/dextromethorphan hydrobromide combination) in the treatment of chronic pain: Three multicenter, randomized, double-blind, controlled clinical trials fail to demonstrate enhanced opioid analgesia or reduction in tolerance. Pain, 115(3), 284–295. https://doi.org/10.1016/j.pain.2005.03.004
Ganetsky, M., Babu, K. M., & Boyer, E. W. (2007). Serotonin Syndrome in Dextromethorphan Ingestion Responsive to Propofol Therapy. Pediatric Emergency Care, 23(11), 829–831. https://doi.org/10.1097/PEC.0b013e31815a0667
George, C. P., Goldberg, M. P., Choi, D. W., & Steinberg, G. K. (1988). Dextromethorphan reduces neocortical ischemic neuronal damage in vivo. Brain Research, 440(2), 375–379. https://doi.org/10.1016/0006-8993(88)91011-6
Gershman, J. A., & Fass, A. D. (2013). Dextromethorphan Abuse: A Literature Review. Journal of Pharmacy Technology, 29(2), 66–71. https://doi.org/10.1177/875512251302900204
Ghasemzadeh, Z., & Rezayof, A. (2016). Role of hippocampal and prefrontal cortical signaling pathways in dextromethorphan effect on morphine-induced memory impairment in rats. Neurobiology of Learning and Memory, 128(December), 23–32. https://doi.org/10.1016/j.nlm.2015.11.015
Ghasemzadeh, Z., & Rezayof, A. (2017). Neuromodulatory effects of the dorsal hippocampal endocannabinoid system in dextromethorphan/morphine-induced amnesia. European Journal of Pharmacology, 794, 100–105. https://doi.org/10.1016/j.ejphar.2016.11.025
Gibaja, V., Boltz, P., Tournebize, J., Labadie, M., Boulamery, A., Villa, A. F., … Kahn, J.-P. (2016). Dextromethorphan intoxications: Data from the French Toxicovigilance and Poison Control Centers from 1999 to 2014. Toxicologie Analytique et Clinique, 28(3), 246–247. https://doi.org/10.1016/j.toxac.2016.05.025
Gilron, I., Booher, S. L., Rowan, M. S., Smoller, M. S., & Max, M. B. (2000). A randomized, controlled trial of high-dose dextromethorphan in facial neuralgias. Neurology, 55(7), 964–71. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/11061252
Goey, A. K. L., Meijerman, I., Beijnen, J. H., & Schellens, J. H. M. (2013). The effect of grape seed extract on the pharmacokinetics of dextromethorphan in healthy volunteers. European Journal of Clinical Pharmacology, 69(11), 1883–1890. https://doi.org/10.1007/s00228-013-1558-9
Gorski, J. C., Jones, D. R., Wrighton, S. A., & Hall, S. D. (1994). Characterization of dextromethorphan N-demethylation by human liver microsomes. Biochemical Pharmacology, 48(1), 173–182. https://doi.org/10.1016/0006-2952(94)90237-2
Grace, R. F., Power, I., Umedaly, H., Zammit, A., Mersiades, M., Cousins, M. J., & Mather, L. E. (1998). Preoperative dextromethorphan reduces intraoperative but not postoperative morphine requirements after laparotomy. Anesthesia and Analgesia, 87(5), 1135–8. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/9806696
Grattan, T., Marshall, A., Higgins, K., & Morice, A. (1995). The effect of inhaled and oral dextromethorphan on citric acid induced cough in man. British Journal of Clinical Pharmacology, 39(3), 261–263. https://doi.org/10.1111/j.1365-2125.1995.tb04446.x
Graudins, A., & Fern, R. P. (1996). Acute Dystonia in a Child Associated with Therapeutic Ingestion of a Dextromethorphan Containing Cough and Cold Syrup. Journal of Toxicology: Clinical Toxicology, 34(3), 351–352. https://doi.org/10.3109/15563659609013802
Hasan, R. A., Kartush, J. M., Thomas, J. D., & Sigler, D. L. (2004). Oral Dextromethorphan Reduces Perioperative Analgesic Administration in Children Undergoing Tympanomastoid Surgery. Otolaryngology-Head and Neck Surgery, 131(5), 711–716. https://doi.org/10.1016/j.otohns.2004.06.709
Henderson, D. J., Withington, B. S., Wilson, J. a, & Morrison, L. M. M. (1999). Perioperative Dextromethorphan Reduces Postoperative Pain After Hysterectomy. Anesthesia & Analgesia, 89(2), 399–402. https://doi.org/10.1213/00000539-199908000-00028
Henderson, M. G., & Fuller, R. W. (1992). Dextromethorphan antagonizes the acute depletion of brain serotonin by p-chloroamphetamine and H75/12 in rats. Brain Research, 594(2), 323–326. https://doi.org/10.1016/0006-8993(92)91144-4
Hendrickson, R. G., & Cloutier, R. L. (2007). “Crystal Dex:” Free-Base Dextromethorphan. The Journal of Emergency Medicine, 32(4), 393–396. https://doi.org/10.1016/j.jemermed.2007.03.010
Hernandez, S. (2000). Dextromethorphan and Its Metabolite Dextrorphan Block α3β4 Neuronal Nicotinic Receptors. Neuropharmacology.
Hinsberger, A., Sharma, V., & Mazmanian, D. (1994). Cognitive deterioration from long-term abuse of dextromethorphan: a case report. Journal of Psychiatry & Neuroscience : JPN, 19(5), 375–7. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/7803371
Hoffmann, O., & Wiesenfeld-Hallin, Z. (1996). Dextromethorphan potentiates morphine antinociception, but does not reverse tolerance in rats. Neuroreport, 7(3), 838–40. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/8733757
Hou, C.-H., Tzeng, J.-I., Chen, Y.-W., Lin, C.-N., Lin, M.-T., Tu, C.-H., & Wang, J.-J. (2006). Dextromethorphan, 3-methoxymorphinan, and dextrorphan have local anaesthetic effect on sciatic nerve blockade in rats. European Journal of Pharmacology, 544(1–3), 10–16. https://doi.org/10.1016/j.ejphar.2006.06.013
Huang, E. Y.-K., Liu, T., & Tao, P. (2003). Co-administration of dextromethorphan with morphine attenuates morphine rewarding effect and related dopamine releases at the nucleus accumbens. Naunyn-Schmiedeberg’s Archives of Pharmacology, 368(5), 386–392. https://doi.org/10.1007/s00210-003-0803-7
Huang, M.-C., Chen, C.-H., Pan, C.-H., & Lin, S.-K. (2014). Lack of Efficacy of Dextromethorphan in Managing Alcohol Withdrawal. Journal of Clinical Psychopharmacology, 34(1), 149–152. https://doi.org/10.1097/JCP.0000000000000052
Ishibashi, H., Kuwano, K., & Takahama, K. (2000). Inhibition of the 5-HT1A receptor-mediated inwardly rectifying K+ current by dextromethorphan in rat dorsal raphe neurones. Neuropharmacology, 39(12), 2302–2308. https://doi.org/10.1016/S0028-3908(00)00092-7
Jamison, S., & Vasudeva, S. (2009). A 60-year-old woman with agitation and psychosis following ingestion of dextromethorphan and opioid analgesics. Journal of Psychopharmacology, 23(8), 989–991. https://doi.org/10.1177/0269881108092125
Jiménez, A., Marin, C., Bonastre, M., & Tolosa, E. (1999). Narrow beneficial effect of dextromethorphan on levodopa-induced motor response alterations in an experimental model of parkinsonism. Brain Research, 839(1), 190–193. https://doi.org/10.1016/S0006-8993(99)01657-1
Jun, J. ., & Schindler, C. . (2000). Dextromethorphan alters methamphetamine self-administration in the rat. Pharmacology Biochemistry and Behavior, 67(3), 405–409. https://doi.org/10.1016/S0091-3057(00)00317-8
Jun, J. H., Thorndike, E. B., & Schindler, C. W. (2004). Abuse liability and stimulant properties of dextromethorphan and diphenhydramine combinations in rats. Psychopharmacology, 172(3), 277–282. https://doi.org/10.1007/s00213-003-1650-4
Kalia, L. V, Kalia, S. K., & Salter, M. W. (2008). NMDA receptors in clinical neurology: excitatory times ahead. The Lancet Neurology, 7(8), 742–755. https://doi.org/10.1016/S1474-4422(08)70165-0
Kamei, H., Kameyama, T., & Nabeshima, T. (1996). (+)-SKF-10,047 and dextromethorphan ameliorate conditioned fear stress through the activation of phenytoin-regulated σ1 sites. European Journal of Pharmacology, 299(1–3), 21–28. https://doi.org/10.1016/0014-2999(95)00830-6
Kamel, I. R., Wendling, W. W., Chen, D., Wendling, K. S., Harakal, C., & Carlsson, C. (2008). N-Methyl-D-Aspartate (NMDA) Antagonists—S(+)-ketamine, Dextrorphan, and Dextromethorphan—Act as Calcium Antagonists on Bovine Cerebral Arteries. Journal of Neurosurgical Anesthesiology, 20(4), 241–248. https://doi.org/10.1097/ANA.0b013e31817f523f
Kelly, T. F., & Lieberman, D. Z. (2014). The utility of the combination of dextromethorphan and quinidine in the treatment of bipolar II and bipolar NOS. Journal of Affective Disorders, 167, 333–335. https://doi.org/10.1016/j.jad.2014.05.050
Kerry, N. L., Somogyi, A. A., Bochner, F., & Mikus, G. (1994). The role of CYP2D6 in primary and secondary oxidative metabolism of dextromethorphan: in vitro studies using human liver microsomes. British Journal of Clinical Pharmacology, 38(3), 243–8. Retrieved from http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=1364796&tool=pmcentrez&rendertype=abstract
Kim, H.-C., Ho Ko, K., Kim, W.-K., Shin, E.-J., Kang, K.-S., Young Shin, C., & Jhoo, W.-K. (2001). Effects of dextromethorphan on the seizures induced by kainate and the calcium channel agonist BAY k-8644: comparison with the effects of dextrorphan. Behavioural Brain Research, 120(2), 169–175. https://doi.org/10.1016/S0166-4328(00)00372-7
Kim, H. C., Bing, G., Shin, E. J., Jhoo, H. S., Cheon, M. A., Lee, S. H., … Jhoo, W. K. (2001). Dextromethorphan affects cocaine-mediated behavioral pattern in parallel with a long-lasting Fos-related antigen-immunoreactivity. Life Sciences, 69(6), 615–24. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/11476183
King, M. R., Ladha, K. S., Gelineau, A. M., & Anderson, T. A. (2016). Perioperative Dextromethorphan as an Adjunct for Postoperative Pain. Anesthesiology, 124(3), 696–705. https://doi.org/10.1097/ALN.0000000000000950
Kinoshita, H., Ohkubo, T., Yasuda, M., & Yakushiji, F. (2011). Serotonin syndrome induced by dextromethorphan (Medicon) administrated at the conventional dose. Geriatrics & Gerontology International, 11(1), 121–122. https://doi.org/10.1111/j.1447-0594.2010.00652.x
Kintz, P., & Mangin, P. (1992). Toxicological Findings in a Death Involving Dextromethorphan and Terfenadine. The American Journal of Forensic Medicine and Pathology, 13(4), 351–352. https://doi.org/10.1097/00000433-199212000-00018
Klein, M., Paturzo, J. J., & Musacchio, J. (1989). The effects of prototypic σ ligands on the binding of [3H]dextromethorphan to guinea pig brain. Neuroscience Letters, 97(1–2), 175–180. https://doi.org/10.1016/0304-3940(89)90159-6
Koyuncuoğlu, H., Güngör, M., Sağduyu, H., & Aricioğlu, F. (1990). Suppression by ketamine and dextromethorphan of precipitated abstinence syndrome in rats. Pharmacology, Biochemistry, and Behavior, 35(4), 829–32. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/2345761
Koyuncuoğlu, H., & Saydam, B. (1990). The treatment of heroin addicts with dextromethorphan: a double-blind comparison of dextromethorphan with chlorpromazine. International Journal of Clinical Pharmacology, Therapy, and Toxicology, 28(4), 147–52. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/2187002
Kuiken, S. D., Lei, A., Tytgat, G. N. J., Holman, R., & Boeckxstaens, G. E. E. (2002). Effect of the low-affinity, noncompetitive N-methyl-d-aspartate receptor antagonist dextromethorphan on visceral perception in healthy volunteers. Alimentary Pharmacology and Therapeutics, 16(11), 1955–1962. https://doi.org/10.1046/j.1365-2036.2002.01358.x
Kung, S. (2007). Serotonin Syndrome With Tramadol and Dextromethorphan. Hong Kong Journal of Emerg, 14(1), 48–52.
L. Zoler, M. (2015). Dextromethorphan/Quinidine Effective for Agitation. Caring for the Ages, 16(9), 1–15. https://doi.org/10.1016/j.carage.2015.08.002
Lauterbach, E. C. (2016). Treatment Resistant Depression with Loss of Antidepressant Response: Rapid-Acting Antidepressant Action of Dextromethorphan, A Possible Treatment Bridging Molecule. Psychopharmacology Bulletin, 46(2), 53–58. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/27738380
Lee, K.-H., Ahn, J.-I., Yu, D.-H., Koh, H. C., Kim, S. H., Yang, B. H., … Lee, Y.-S. (2003). Dextromethorphan alters gene expression in rat brain hippocampus and cortex. International Journal of Molecular Medicine, 11(5), 559–68. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/12684690
Lee, S.-Y., Chen, S.-L., Chang, Y.-H., Chen, S.-H., Chu, C.-H., Huang, S.-Y., … Lu, R.-B. (2012). The DRD2/ANKK1 gene is associated with response to add-on dextromethorphan treatment in bipolar disorder. Journal of Affective Disorders, 138(3), 295–300. https://doi.org/10.1016/j.jad.2012.01.024
Lee, S.-Y., Chen, S.-L., Chang, Y.-H., Chu, C.-H., Chen, S.-H., Chen, P. S., … Lu, R.-B. (2015). A Placebo-Controlled Trial of Dextromethorphan as an Adjunct in Opioid-Dependent Patients Undergoing Methadone Maintenance Treatment. International Journal of Neuropsychopharmacology, 18(7), pyv008-pyv008. https://doi.org/10.1093/ijnp/pyv008
Lee, S.-Y., Chen, S.-L., Chang, Y., Chen, P.-S., Huang, S., Tzeng, N., … Lu, R.-B. (2015). ALDH2 polymorphism, associated with attenuating negative symptoms in patients with schizophrenia treated with add-on dextromethorphan. Journal of Psychiatric Research, 69, 50–56. https://doi.org/10.1016/j.jpsychires.2015.07.027
Lee, S.-Y., Chen, S.-L., Wang, T.-Y., Chang, Y.-H., Chen, P. S., Huang, S.-Y., … Lu, R.-B. (2017). The COMT Val158Met Polymorphism Is Associated With Response to Add-on Dextromethorphan Treatment in Bipolar Disorder. Journal of Clinical Psychopharmacology, 37(1), 94–98. https://doi.org/10.1097/JCP.0000000000000633
Lee PCL, Jawad, M. S., & Eccles, R. (2000). Antitussive efficacy of dextromethorphan in cough associated with acute upper respiratory tract infection. The Journal of Pharmacy and Pharmacology, 52(9), 1137–42. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/11045895
Li, G. (2005). Femtomolar concentrations of dextromethorphan protect mesencephalic dopaminergic neurons from inflammatory damage. The FASEB Journal, 19(6), 489–496. https://doi.org/10.1096/fj.04-2555com
Li, G., Liu, Y., Tzeng, N., Cui, G., Block, M. L., Wilson, B., … Hong, J.-S. (2005). Protective effect of dextromethorphan against endotoxic shock in mice. Biochemical Pharmacology, 69(2), 233–240. https://doi.org/10.1016/j.bcp.2004.10.003
Lin, S., Pan, C.-H., & Chen, C. (2014). A Double-Blind, Placebo-Controlled Trial of Dextromethorphan Combined With Clonidine in the Treatment of Heroin Withdrawal. Journal of Clinical Psychopharmacology, 34(4), 508–512. https://doi.org/10.1097/JCP.0000000000000144
Lisak, R. P., Nedelkoska, L., & Benjamins, J. A. (2014). Effects of dextromethorphan on glial cell function: Proliferation, maturation, and protection from cytotoxic molecules. Glia, 62(5), 751–762. https://doi.org/10.1002/glia.22639
LIU, P.-Y., LIN, C.-C., TSAI, W.-C., LI, Y.-H., LIN, L.-J., SHI, G.-Y., … WU, H.-L. (2008). Treatment with dextromethorphan improves endothelial function, inflammation and oxidative stress in male heavy smokers. Journal of Thrombosis and Haemostasis, 6(10), 1685–1692. https://doi.org/10.1111/j.1538-7836.2008.03082.x
Liu, Y. (2003). Dextromethorphan Protects Dopaminergic Neurons against Inflammation-Mediated Degeneration through Inhibition of Microglial Activation. Journal of Pharmacology and Experimental Therapeutics, 305(1), 212–218. https://doi.org/10.1124/jpet.102.043166
Logan, B. K., Goldfogel, G., Hamilton, R., & Kuhlman, J. (2009). Five deaths resulting from abuse of dextromethorphan sold over the internet. Journal of Analytical Toxicology, 33(2), 99–103. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/19239735
Logan, B. K., Yeakel, J. K., Goldfogel, G., Frost, M. P., Sandstrom, G., & Wickham, D. J. (2012). Dextromethorphan Abuse Leading to Assault, Suicide, or Homicide. Journal of Forensic Sciences, 57(5), 1388–1394. https://doi.org/10.1111/j.1556-4029.2012.02133.x
Lotrich, F. E., Rosen, J., & Pollock, B. G. (2005). Dextromethorphan-induced delirium and possible methadone interaction. The American Journal of Geriatric Pharmacotherapy, 3(1), 17–20. https://doi.org/10.1016/].amjopharm.2005.03.002
LoVecchio, F., Pizon, A., Matesick, L., & O’Patry, S. (2008). Accidental dextromethorphan ingestions in children less than 5 years old. Journal of Medical Toxicology : Official Journal of the American College of Medical Toxicology, 4(4), 251–3. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/19031376
Lue, W.-M., Huang, E. Y.-K., Yang, S.-N., Wong, C.-S., & Tao, P.-L. (2007). Post-treatment of dextromethorphan reverses morphine effect on conditioned place preference in rats. Synapse, 61(6), 420–428. https://doi.org/10.1002/syn.20391
Ma, K., Liu, T., Weng, S., Chen, C. F., Huang, Y., Chueh, S., … Cheng, C. (2016). Effects of dextromethorphan on MDMA-induced serotonergic aberration in the brains of non- human primates using [ 123 I ] -ADAM /. Nature Publishing Group, (December), 4–11. https://doi.org/10.1038/srep38695
Madeira, J., Schindler, S., & Klegeris, A. (2015). A new look at auranofin, dextromethorphan and rosiglitazone for reduction of glia-mediated inflammation in neurodegenerative diseases. Neural Regeneration Research, 10(3), 391. https://doi.org/10.4103/1673-5374.153686
Majlesi, N., Lee, D. C., & Ali, S. S. (2011). Dextromethorphan Abuse Masquerading as a Recurrent Seizure Disorder. Pediatric Emergency Care, 27(3), 210–211. https://doi.org/10.1097/PEC.0b013e31820d8dc1
Malek, A., Amiri, S., & Habibi Asl, B. (2013). The Therapeutic Effect of Adding Dextromethorphan to Clonidine for Reducing Symptoms of Opioid Withdrawal: A Randomized Clinical Trial. ISRN Psychiatry, 2013, 1–5. https://doi.org/10.1155/2013/546030
Manaboriboon, B., & Chomchai, C. (2005). Dextromethorphan abuse in Thai adolescents: A report of two cases and review of literature. Journal of the Medical Association of Thailand = Chotmaihet Thangphaet, 88 Suppl 8, S242-5. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/16856446
Many, S. (1992). Dextromethorphan & Brief Delusional Psychosis: Case Report. Retrieved from http://smpsych.com/cases/case1.pdf
Mao, J., Price, D. D., Caruso, F. S., & Mayer, D. J. (1996). Oral administration of dextromethorphan prevents the development of morphine tolerance and dependence in rats. Pain, 67(2), 361–368. https://doi.org/10.1016/0304-3959(96)03120-X
Marashi, S. M. (2013). Suppressing Effect of Dextromethorphan or Clonidine on Fentanyl- Induced Coughing: A Double- Blind, Prospective, Randomized Placebo- Controlled Study. Journal of Pulmonary & Respiratory Medicine, 3(3), 216. https://doi.org/10.4172/2161-105X.1000150
Marinetti, L., Lehman, L., Casto, B., Harshbarger, K., Kubiczek, P., & Davis, J. (2005). Over-the-Counter Cold Medications–Postmortem Findings in Infants and the Relationship to Cause of Death. Journal of Analytical Toxicology, 29(7), 738–743. https://doi.org/10.1093/jat/29.7.738
Marquard, J., Otter, S., Welters, A., Stirban, A., Fischer, A., Eglinger, J., … Lammert, E. (2015). Characterization of pancreatic NMDA receptors as possible drug targets for diabetes treatment. Nature Medicine, 21(4), 363–372. https://doi.org/10.1038/nm.3822
Marquard, J., Stirban, A., Schliess, F., Sievers, F., Welters, A., Otter, S., … Lammert, E. (2016). Effects of dextromethorphan as add-on to sitagliptin on blood glucose and serum insulin concentrations in individuals with type 2 diabetes mellitus: a randomized, placebo-controlled, double-blinded, multiple crossover, single-dose clinical trial. Diabetes, Obesity and Metabolism, 18(1), 100–103. https://doi.org/10.1111/dom.12576
Marquard, J., Stirban, A., Schliess, F., Sievers, F., Welters, A., Otter, S., … Lammert, E. (2016). Effects of dextromethorphan as add-on to sitagliptin on blood glucose and serum insulin concentrations in individuals with type 2 diabetes mellitus: a randomized, placebo-controlled, double-blinded, multiple crossover, single-dose clinical trial. Diabetes, Obesity and Metabolism, 18(1), 100–103. https://doi.org/10.1111/dom.12576
Martinak, B., Bolis, R. A., Black, J. R., Fargason, R. E., & Birur, B. (2017). Dextromethorphan in Cough Syrup: The Poor Man’s Psychosis. Psychopharmacology Bulletin, 47(4), 59–63. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5601090/pdf/PB-47-4-59.pdf
MATIN, N., KURANI, A., KENNEDY, C., & LIU, Q. (2007). Dextromethorphan-induced near-fatal suicide attempt in a slow metabolizer at cytochrome P450 2D6. The American Journal of Geriatric Pharmacotherapy, 5(2), 162–165. https://doi.org/10.1016/j.amjopharm.2007.05.001
Matthys, H., Bleicher, B., & Bleicher, U. (1983). Dextromethorphan and Codeine: Objective Assessment of Antitussive Activity in Patients with Chronic Cough. Journal of International Medical Research, 11(2), 92–100. https://doi.org/10.1177/030006058301100206
McFee, R. B., Mofenson, H. C., & Caraccio, T. R. (2000). Dextromethorphan: another “ecstasy”? Archives of Family Medicine, 9(2), 123. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/10693726
McQuay, H. J., Carroll, D., Jadad, A. R., Glynn, C. J., Jack, T., Moore, A. R., & Wiffen, P. J. (1994). Dextromethorphan for the treatment of neuropathic pain: a double-blind randomised controlled crossover trial with integral n-of-1 design. Pain, 59(1), 127–133. https://doi.org/10.1016/0304-3959(94)90056-6
Mercadante, S., Casuccio, A., & Genovese, G. (1998). Ineffectiveness of Dextromethorphan in Cancer Pain. Journal of Pain and Symptom Management, 16(5), 317–322. https://doi.org/10.1016/S0885-3924(98)00096-7
Messias, E., & Everett, B. (2012). Dextromethorphan and Quinidine Combination in Emotional Lability Associated With Depression. The Primary Care Companion For CNS Disorders, 14(5), . Epub 2012 Oct 25 doi:10.4088/PCC.12l01400. https://doi.org/10.4088/PCC.12l01400
Metman, L. V., Blanchet, P. J., van den Munckhof, P., Dotto, P. Del, Natté, R., & Chase, T. N. (1998). A trial of dextromethorphan in parkinsonian patients with motor response complications. Movement Disorders, 13(3), 414–417. https://doi.org/10.1002/mds.870130307
Miller, A., & Panitch, H. (2007). Therapeutic use of dextromethorphan: Key learnings from treatment of pseudobulbar affect. Journal of the Neurological Sciences, 259(1–2), 67–73. https://doi.org/10.1016/j.jns.2006.06.030
Miller, S. (2005). Dextromethorphan psychosis, dependence and physical withdrawal. Addiction Biology, 10(4), 325–327. https://doi.org/10.1080/13556210500352410
Miller, S. C. (2011). Dextromethorphan to dextrorphan: a pathway towards abuse liability. Human Psychopharmacology: Clinical and Experimental, 26(1), 89–90. https://doi.org/10.1002/hup.1164
Modi, D., Bhalavat, R., & Patterson, J. C. (2013). Suicidal and Homicidal Behaviors Related to Dextromethorphan Abuse in a Middle-Aged Woman. Journal of Addiction Medicine, 7(2), 143–144. https://doi.org/10.1097/ADM.0b013e318281a547
Montastruc, J. L., Fabre, N., Rascol, O., Senard, J. M., & Blin, O. (2004). N-methyl-D-aspartate (NMDA) antagonist and Parkinson’s disease: A pilot study with dextromethorphan. Movement Disorders, 9(2), 242–243. https://doi.org/10.1002/mds.870090226
Monte, A. A., Chuang, R., & Bodmer, M. (2010). Dextromethorphan, chlorphenamine and serotonin toxicity: case report and systematic literature review. British Journal of Clinical Pharmacology, 70(6), 794–798. https://doi.org/10.1111/j.1365-2125.2010.03747.x
Morel, V., Pickering, G., Etienne, M., Dupuis, A., Privat, A.-M., Chalus, M., … Daulhac, L. (2014). Low doses of dextromethorphan have a beneficial effect in the treatment of neuropathic pain. Fundamental & Clinical Pharmacology, 28(6), 671–680. https://doi.org/10.1111/fcp.12076
Morris, H., & Wallach, J. (2014). From PCP to MXE: a comprehensive review of the non-medical use of dissociative drugs. Drug Testing and Analysis, 6(7–8), 614–632. https://doi.org/10.1002/dta.1620
Mousavi, S. A., Saadatnia, M., Khorvash, F., Hoseini, T., & Sariaslani, P. (2011). Evaluation of the neuroprotective effect of dextromethorphan in the acute phase of ischaemic stroke. Archives of Medical Science, 3, 465–469. https://doi.org/10.5114/aoms.2011.23413
Murray, S., & Brewerton, T. (1993). Abuse of over-the-counter dextromethorphan by teenagers. Southern Medical Journal, 86(10), 1151–3. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/8211334
Murrough, J. W., Wade, E., Sayed, S., Ahle, G., Kiraly, D. D., Welch, A., … Charney, D. S. (2017). Dextromethorphan/quinidine pharmacotherapy in patients with treatment resistant depression: A proof of concept clinical trial. Journal of Affective Disorders, 218, 277–283. https://doi.org/10.1016/j.jad.2017.04.072
Mutschler, J., Koopmann, A., Grosshans, M., Hermann, D., Mann, K., & Kiefer, F. (2010). Dextromethorphan Withdrawal and Dependence Syndrome. Deutsches Aerzteblatt Online, 107(30), 537–540. https://doi.org/10.3238/arztebl.2010.0537
Nam, Y., Shin, E.-J., Yang, B.-K., Bach, J.-H., Jeong, J. H., Chung, Y. H., … Kim, H.-C. (2012). Dextromethorphan-induced psychotoxic behaviors cause sexual dysfunction in male mice via stimulation of σ-1 receptors. Neurochemistry International, 61(6), 913–922. https://doi.org/10.1016/j.neuint.2012.01.025
Nelson, K. a, Park, K. M., Robinovitz, E., Tsigos, C., & Max, M. B. (1997). High-dose oral dextromethorphan versus placebo in painful diabetic neuropathy and postherpetic neuralgia. Neurology. https://doi.org/10.1212/WNL.48.5.1212
Ng, Y.-Y., Lin, W.-L., Chen, T.-W., Lin, B.-C., Tsai, S.-H., Chang, C.-C., & Huang, T.-P. (1992). Spurious Hyperchloremia and Decreased Anion Gap in a Patient with Dextromethorphan Bromide. American Journal of Nephrology, 12(4), 268–270. https://doi.org/10.1159/000168457
Nguyen, L., Lucke-Wold, B. P., Logsdon, A. F., Scandinaro, A. L., Huber, J. D., & Matsumoto, R. R. (2016). Behavioral and biochemical effects of ketamine and dextromethorphan relative to its antidepressant-like effects in Swiss Webster mice. NeuroReport, 27(14), 1004–1011. https://doi.org/10.1097/WNR.0000000000000646
Nguyen, L., & Matsumoto, R. R. (2015). Involvement of AMPA receptors in the antidepressant-like effects of dextromethorphan in mice. Behavioural Brain Research, 295, 26–34. https://doi.org/10.1016/j.bbr.2015.03.024
Nguyen, L., Robson, M. J., Healy, J. R., Scandinaro, A. L., & Matsumoto, R. R. (2014). Involvement of Sigma-1 Receptors in the Antidepressant-like Effects of Dextromethorphan. PLoS ONE, 9(2), e89985. https://doi.org/10.1371/journal.pone.0089985
Nguyen, L., Scandinaro, A. L., & Matsumoto, R. R. (2017). Deuterated (d6)-dextromethorphan elicits antidepressant-like effects in mice. Pharmacology Biochemistry and Behavior, 161(April), 30–37. https://doi.org/10.1016/j.pbb.2017.09.005
Okland, T., Shirazi, M., Rylander, M., & Holland, J. (2016). A Case of Aggressive Psychosis in the Setting of Regular Dextromethorphan Abuse. Psychosomatics, 57(6), 655–656. https://doi.org/10.1016/j.psym.2016.06.002
P. Witter, D., Ramnaraine, L., & A. Shapiro, M. (2016). A Possible Case of Bipolar Disorder Unmasked by Dextromethorphan in a 16-year-old Adolescent. Adolescent Psychiatry, 5(4), 273–276. https://doi.org/10.2174/2210676606666160502130909
Panitch, H. S., Thisted, R. A., Smith, R. A., Wynn, D. R., Wymer, J. P., Achiron, A., … Miller, A. (2006). Randomized, controlled trial of dextromethorphan/quinidine for pseudobulbar affect in multiple sclerosis. Annals of Neurology, 59(5), 780–787. https://doi.org/10.1002/ana.20828
Pattee, G. L., Wymer, J. P., Lomen-Hoerth, C., Appel, S. H., Formella, A. E., & Pope, L. E. (2014). An open-label multicenter study to assess the safety of dextromethorphan/quinidine in patients with pseudobulbar affect associated with a range of underlying neurological conditions. Current Medical Research and Opinion, 30(11), 2255–2265. https://doi.org/10.1185/03007995.2014.940040
Paul, I. M. (2007). Effect of Honey, Dextromethorphan, and No Treatment on Nocturnal Cough and Sleep Quality for Coughing Children and Their Parents. Archives of Pediatrics & Adolescent Medicine, 161(12), 1140. https://doi.org/10.1001/archpedi.161.12.1140
Paul, I. M., Reynolds, K. M., Kauffman, R. E., Banner, W., Bond, G. R., Palmer, R. B., … Green, J. L. (2017). Adverse events associated with pediatric exposures to dextromethorphan. Clinical Toxicology, 55(1), 25–32. https://doi.org/10.1080/15563650.2016.1240803
Paul, I. M., Yoder, K. E., Crowell, K. R., Shaffer, M. L., McMillan, H. S., Carlson, L. C., … Berlin, C. M. (2004). Effect of dextromethorphan, diphenhydramine, and placebo on nocturnal cough and sleep quality for coughing children and their parents. Pediatrics, 114(1), e85-90. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/15231978
Pechnick, R. N. (2004). Comparison of the Effects of Dextromethorphan, Dextrorphan, and Levorphanol on the Hypothalamo-Pituitary-Adrenal Axis. Journal of Pharmacology and Experimental Therapeutics, 309(2), 515–522. https://doi.org/10.1124/jpet.103.060038
Pender, E. S., & Parks, B. R. (1991). Toxicity with dextromethorphan-containing preparations: a literature review and report of two additional cases. Pediatric Emergency Care, 7(3), 163–5. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/1876508
Perry, P. J., Fredriksen, K., Chew, S., Ip, E. J., Lopes, I., Doroudgar, S., & Thomas, K. (2015). The Effects of Dextromethorphan on Driving Performance and the Standardized Field Sobriety Test. Journal of Forensic Sciences, 60(5), 1258–1262. https://doi.org/10.1111/1556-4029.12833
Plesan, A., Hedman, U., Xu, X. J., & Wiesenfeld-Hallin, Z. (1998). Comparison of ketamine and dextromethorphan in potentiating the antinociceptive effect of morphine in rats. Anesthesia and Analgesia, 86(4), 825–9. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/9539609
Po, K. T., Siu, A. M.-H., Lau, B. W.-M., Chan, J. N.-M., So, K.-F., & Chan, C. C. H. (2015). Repeated, high-dose dextromethorphan treatment decreases neurogenesis and results in depression-like behavior in rats. Experimental Brain Research, 233(7), 2205–2214. https://doi.org/10.1007/s00221-015-4290-0
Polles, A. (1996). Case Reports Dextromethorphan-Induced Mania. Psychosomatics, 37(1), 71–74. https://doi.org/10.1016/S0033-3182(96)71601-8
Pope, L. E., Khalil, M. H., Berg, J. E., Stiles, M., Yakatan, G. J., & Sellers, E. M. (2004). Pharmacokinetics of Dextromethorphan After Single or Multiple Dosing in Combination With Quinidine in Extensive and Poor Metabolizers. The Journal of Clinical Pharmacology, 44(10), 1132–1142. https://doi.org/10.1177/0091270004269521
Posod, A., Pinzer, K., Urbanek, M., Wegleiter, K., Keller, M., Kiechl-Kohlendorfer, U., & Griesmaier, E. (2014). The common antitussive agent dextromethorphan protects against hyperoxia-induced cell death in established in vivo and in vitro models of neonatal brain injury. Neuroscience, 274, 260–272. https://doi.org/10.1016/j.neuroscience.2014.05.059
Price, D. D., Mao, J., Lu, J., Caruso, F. S., Frenk, H., & Mayer, D. J. (1996). Effects of the combined oral administration of NSAIDs and dextromethorphan on behavioral symptoms indicative of arthritic pain in rats. Pain, 68(1), 119–27. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/9252006
Price, L. (2000). Dextromethorphan-Induced Psychosis, (1).
Pringle, G., McDonald, M. P., & Gabriel, K. I. (2015). Patterns and Perceptions of Dextromethorphan Use in Adult Members of an Online Dextromethorphan Community. Journal of Psychoactive Drugs, 47(4), 267–275. https://doi.org/10.1080/02791072.2015.1071448
PT687. Dextromethorphan-induced serotonin syndrome requires activation of protein kinase C- d gene. (2016). International Journal of Neuropsychopharmacology, 19(Suppl_1), 50–50. https://doi.org/10.1093/ijnp/pyw044.687
PU, B., XUE, Y., WANG, Q., HUA, C., & LI, X. (2015). Dextromethorphan provides neuroprotection via anti-infammatory and anti-excitotoxicity effects in the cortex following traumatic brain injury. Molecular Medicine Reports, 12(3), 3704–3710. https://doi.org/10.3892/mmr.2015.3830
Pulvirenti, L., Balducci, C., & Koob, G. F. (1997). Dextromethorphan reduces intravenous cocaine self-administration in the rat. European Journal of Pharmacology, 321(3), 279–83. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/9085038
Qiu, Y., Lv, X., Jiang, G., Su, H.-H., Ma, X., Tian, J., & Zhuo, F. (2017). Potential gray matter unpruned in adolescents and young adults dependent on dextromethorphan-containing cough syrups: evidence from cortical and subcortical study. Brain Imaging and Behavior, 11(5), 1470–1478. https://doi.org/10.1007/s11682-016-9628-0
Rammer, L., Holmgren, P., & Sandler, H. (1988). Fatal intoxication by dextromethorphan: a report on two cases. Forensic Science International, 37(4), 233–6. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/3410392
Ramsay, J., Wright, C., Thompson, R., Hull, D., & Morice, A. H. (2008). Assessment of antitussive efficacy of dextromethorphan in smoking related cough: objective vs. subjective measures. British Journal of Clinical Pharmacology, 65(5), 737–741. https://doi.org/10.1111/j.1365-2125.2008.03115.x
Reissig, C. J., Carter, L. P., Johnson, M. W., Mintzer, M. Z., Klinedinst, M. A., & Griffiths, R. R. (2012). High doses of dextromethorphan, an NMDA antagonist, produce effects similar to classic hallucinogens. Psychopharmacology, 223(1), 1–15. https://doi.org/10.1007/s00213-012-2680-6
Rivers, N., & Horner, B. (1970). Possible lethal reaction between nardil and dextromethorphan. Canadian Medical Association Journal, 103(1), 85. https://doi.org/http://dx.doi.org/10.1016/0346-251X(90)90045-7
Robertson, S. (2016). Do over-the-counter remedies relieve cough in acute upper respiratory infections? Evidence-Based Practice, 19(9), 1–2.
Romanelli, F., & Smith, K. M. (2009). Dextromethorphan abuse: Clinical effects and management. Journal of the American Pharmacists Association, 49(2), e20–e27. https://doi.org/10.1331/JAPhA.2009.08091
Rosen, M. I., McMahon, T. J., Woods, S. W., Pearsall, H. R., & Kosten, T. R. (1996). A pilot study of dextromethorphan in naloxone-precipitated opiate withdrawal. European Journal of Pharmacology, 307(3), 251–7. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/8836612
Roy, A. K., Hsieh, C., & Crapanzano, K. (2015). Dextromethorphan Addiction Mediated Through the NMDA System. Journal of Addiction Medicine, 9(6), 499–501. https://doi.org/10.1097/ADM.0000000000000152
Salehi, M., Zargar, A., & Ramezani, M. A. (2011). Effects of Dextromethorphan on reducing methadone dosage in opium addicts undergoing methadone maintenance therapy: A double blind randomized clinical trial. Journal of Research in Medical Sciences : The Official Journal of Isfahan University of Medical Sciences, 16(10), 1354–60. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/22973331
Schmider, J., Greenblatt, D. J., Fogelman, S. M., von Moltke, L. L., & Shader, R. I. (1997). Metabolism of dextromethorphan in vitro: involvement of cytochromes P450 2D6 and 3A3/4, with a possible role of 2E1. Biopharmaceutics & Drug Disposition, 18(3), 227–40. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/9113345
Schneider, S. M., Michelson, E. A., Boucek, C. D., & Ilkhanipour, K. (1991). Dextromethorphan poisoning reversed by naloxone. The American Journal of Emergency Medicine, 9(3), 237–8. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/2018593
Schoedel, K., Morrow, S., & Sellers, E. (2014). Evaluating the safety and efficacy of dextromethorphan/quinidine in the treatment of pseudobulbar affect. Neuropsychiatric Disease and Treatment, 10, 1161. https://doi.org/10.2147/NDT.S30713
Schroeder, K., & Fahey, T. (2002). Should we advise parents to administer over the counter cough medicines for acute cough? Systematic review of randomised controlled trials. Archives of Disease in Childhood, 86(3), 170–5. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/11861232
Schwartz, A. R., Pizon, A. F., & Brooks, D. E. (2008). Dextromethorphan-induced serotonin syndrome. Clinical Toxicology, 46(8), 771–773. https://doi.org/10.1080/15563650701668625
Schwartz, R. H. (2005). Adolescent Abuse of Dextromethorphan. Clinical Pediatrics, 44(7), 565–568. https://doi.org/10.1177/000992280504400702
Sethi, R., Kablinger, A. S., & Kavuru, B. (2012). Serotonin Syndrome in a Sertraline-Treated Man Taking NyQuil Containing Dextromethorphan for Cold. The Primary Care Companion For CNS Disorders. https://doi.org/10.4088/PCC.12l01388
Shadkam, M. N., Mozaffari-Khosravi, H., & Mozayan, M. R. (2010). A Comparison of the Effect of Honey, Dextromethorphan, and Diphenhydramine on Nightly Cough and Sleep Quality in Children and Their Parents. The Journal of Alternative and Complementary Medicine, 16(7), 787–793. https://doi.org/10.1089/acm.2009.0311
Shafi, H., Imran, M., Usman, H. F., Sarwar, M., Tahir, M. A., Naveed, R., … Tahir, A. M. (2016). Deaths due to abuse of dextromethorphan sold over-the-counter in Pakistan. Egyptian Journal of Forensic Sciences, 6(3), 280–283. https://doi.org/10.1016/j.ejfs.2015.07.002
SHIN, E., NAH, S., CHAE, J., BING, G., SHIN, S., YEN, T., … NABESHIMA, T. (2007). Dextromethorphan attenuates trimethyltin-induced neurotoxicity via σ1 receptor activation in rats. Neurochemistry International, 50(6), 791–799. https://doi.org/10.1016/j.neuint.2007.01.008
SINCLAIR, J. G. (1973). Dextromethorphan-monoamine oxidase inhibitor interaction in rabbits. Journal of Pharmacy and Pharmacology, 25(10), 803–808. https://doi.org/10.1111/j.2042-7158.1973.tb09945.x
Small, E., & Sandefur, B. J. (2014). Acute Renal Failure after Ingestion of Guaifenesin and Dextromethorphan. The Journal of Emergency Medicine, 47(1), 26–29. https://doi.org/10.1016/j.jemermed.2014.01.022
Smith-Hicks, C. L., Gupta, S., Ewen, J. B., Hong, M., Kratz, L., Kelley, R., … Naidu, S. (2017). Randomized open-label trial of dextromethorphan in Rett syndrome. Neurology, 89(16), 1684–1690. https://doi.org/10.1212/WNL.0000000000004515
Smith, R. A. (2006). Dextromethorphan/quinidine: a novel dextromethorphan product for the treatment of emotional lability. Expert Opinion on Pharmacotherapy, 7(18), 2581–2598. https://doi.org/10.1517/14656566.7.18.2581
Stahl, S. M. (2013). Mechanism of action of dextromethorphan/quinidine: comparison with ketamine. CNS Spectrums, 18(5), 225–227. https://doi.org/10.1017/S109285291300062X
Stanciu, C. N., & Penders, T. M. (2015). Mania after misuse of dextromethorphan: A case report and brief review of “Robotripping.” Journal of Addiction Medicine, 9(2), 159–160. https://doi.org/10.1097/ADM.0000000000000104
Steinberg, G. K., Bell, T. E., & Yenari, M. A. (1996). Dose escalation safety and tolerance study of the N -methyl- d -aspartate antagonist dextromethorphan in neurosurgery patients. Journal of Neurosurgery, 84(5), 860–866. https://doi.org/10.3171/jns.1996.84.5.0860
Steinberg, G. K., Saleh, J., & Kunis, D. (1988). Delayed treatment with dextromethorphan and dextrorphan reduces cerebral damage after transient focal ischemia. Neuroscience Letters, 89(2), 193–7. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/3292967
Strauch, K., Lutz, U., Bittner, N., & Lutz, W. K. (2009). Dose–response relationship for the pharmacokinetic interaction of grapefruit juice with dextromethorphan investigated by human urinary metabolite profiles. Food and Chemical Toxicology, 47(8), 1928–1935. https://doi.org/10.1016/j.fct.2009.05.004
Székely, J. I., Sharpe, L. G., & Jaffe, J. H. (1991). Induction of phencyclidine-like behavior in rats by dextrorphan but not dextromethorphan. Pharmacology, Biochemistry, and Behavior, 40(2), 381–6. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/1805242
Taylor, C. P., Traynelis, S. F., Siffert, J., Pope, L. E., & Matsumoto, R. R. (2016). Pharmacology of dextromethorphan: Relevance to dextromethorphan/quinidine (Nuedexta®) clinical use. Pharmacology & Therapeutics, 164, 170–182. https://doi.org/10.1016/j.pharmthera.2016.04.010
Thomas, D. M., & Kuhn, D. M. (2005). MK-801 and dextromethorphan block microglial activation and protect against methamphetamine-induced neurotoxicity. Brain Research, 1050(1–2), 190–198. https://doi.org/10.1016/j.brainres.2005.05.049
Thompson, C. A. (2010). Oral drug approved for relapsing multiple sclerosis. American Journal of Health-System Pharmacy, 67(21), 1788–1788. https://doi.org/10.2146/news100070
Tortella, F. C., Martin, D. A., Allot, C. P., Steel, J. A., Blackburn, T. P., Loveday, B. E., & Russell, N. J. (1989). Dextromethorphan attenuates post-ischemic hypoperfusion following incomplete global ischemia in the anesthetized rat. Brain Research, 482(1), 179–183. https://doi.org/10.1016/0006-8993(89)90558-1
Tortella, F. C., & Musacchio, J. M. (1986). Dextromethorphan and carbetapentane: centrally acting non-opioid antitussive agents with novel anticonvulsant properties. Brain Research, 383(1–2), 314–8. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/3768695
Tran, H.-Q. (2016). PT686. Dextromethorphan-induced serotonin syndrome is via up-regulation of 5-HT1A receptors. International Journal of Neuropsychopharmacology, 19(Suppl_1), 49–50. https://doi.org/10.1093/ijnp/pyw044.686
Tran, H., Chung, Y. H., Shin, E., Kim, W. K., Lee, J., Jeong, J. H., … Kim, H.-C. (2016). High-dose dextromethorphan produces myelinoid bodies in the hippocampus of rats. Journal of Pharmacological Sciences, 132(2), 166–170. https://doi.org/10.1016/j.jphs.2016.10.001
Verhagen Metman, L., Del Dotto, P., Natté, R., van den Munckhof, P., & Chase, T. N. (1998). Dextromethorphan improves levodopa-induced dyskinesias in Parkinson’s disease. Neurology, 51(1), 203–6. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/9674803
Walker, F. O., & Hunt, V. P. (1989). An open label trial of dextromethorphan in Huntington’s disease. Clinical Neuropharmacology, 12(4), 322–30. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/2529964
Walker, J., & Yatham, L. N. (1993). Benylin (dextromethorphan) abuse and mania. BMJ (Clinical Research Ed.), 306(6882), 896. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/8490415
Wang, S., Zhang, L., Lim, G., Sung, B., Tian, Y., Chou, C., … Mao, J. (2009). A combined effect of dextromethorphan and melatonin on neuropathic pain behavior in rats. Brain Research, 1288, 42–49. https://doi.org/10.1016/j.brainres.2009.06.094
Weinbroum, A. A., Gorodetzky, A., Nirkin, A., Kollender, Y., Bickels, J., Marouani, N., … Meller, I. (2002). Dextromethorphan for the reduction of immediate and late postoperative pain and morphine consumption in orthopedic oncology patients. Cancer, 95(5), 1164–1170. https://doi.org/10.1002/cncr.10784
Weinbroum, A. A., Gorodezky, A., Niv, D., Ben-Abraham, R., Rudick, V., & Szold, A. (2001). Dextromethorphan attenuation of postoperative pain and primary and secondary thermal hyperalgesia. Canadian Journal of Anesthesia/Journal Canadien D’anesthésie, 48(2), 167–174. https://doi.org/10.1007/BF03019730
Weinbroum, A. A., Lalayev, G., Yashar, T., Ben-Abraham, R., Niv, D., & Flaishon, R. (2001). Combined pre-incisional oral dextromethorphan and epidural lidocaine for postoperative pain reduction and morphine sparing: a randomised double-blind study on day-surgery patients. Anaesthesia, 56(7), 616–622. https://doi.org/10.1046/j.1365-2044.2001.02088.x
Welch, L., & Sovner, R. (1992). The treatment of a chronic organic mental disorder with dextromethorphan in a man with severe mental retardation. The British Journal of Psychiatry : The Journal of Mental Science, 161(week 26), 118–20. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/1638308
Werling, L. L., Keller, A., Frank, J. G., & Nuwayhid, S. J. (2007). A comparison of the binding profiles of dextromethorphan, memantine, fluoxetine and amitriptyline: Treatment of involuntary emotional expression disorder. Experimental Neurology, 207(2), 248–257. https://doi.org/10.1016/j.expneurol.2007.06.013
Werling, L. L., Lauterbach, E. C., & Calef, U. (2007). Dextromethorphan as a Potential Neuroprotective Agent With Unique Mechanisms of Action. The Neurologist, 13(5), 272–293. https://doi.org/10.1097/NRL.0b013e3180f60bd8
Wieser, H. G., & Beck, H. (1992). Improvement of medically refractory temporal lobe epilepsy with dextromethorphan. Journal of Epilepsy, 5(4), 246–247. https://doi.org/10.1016/S0896-6974(05)80124-0
Wilson, M. D., Ferguson, R. W., Mazer, M. E., & Litovitz, T. L. (2011). Monitoring trends in dextromethorphan abuse using the National Poison Data System: 2000–2010. Clinical Toxicology, 49(5), 409–415. https://doi.org/10.3109/15563650.2011.585429
Wise, J. (2015). Combination drug shows promise for treating agitation in patients with Alzheimer’s disease. BMJ, 351(September), h5015. https://doi.org/10.1136/bmj.h5015
Wolfe, T. R., & Caravati, E. M. (1995). Massive dextromethorphan ingestion and abuse. The American Journal of Emergency Medicine, 13(2), 174–176. https://doi.org/10.1016/0735-6757(95)90088-8
Wong, B. Y., Coulter, D. A., Choi, D. W., & Prince, D. A. (1988). Dextrorphan and dextromethorphan, common antitussives, are antiepileptic and antagonize N-methyl-d-aspartate in brain slices. Neuroscience Letters, 85(2), 261–266. https://doi.org/10.1016/0304-3940(88)90362-X
Woodard, C., Groden, J., Goodwin, M., Shanower, C., & Bianco, J. (2005). The Treatment of the Behavioral Sequelae of Autism with Dextromethorphan: A Case Report. Journal of Autism and Developmental Disorders, 35(4), 515–518. https://doi.org/10.1007/s10803-005-5041-z
Wright, J., Bond, C., Robertson, H. D., & Matheson, C. (2015). Changes in over-the-counter drug misuse over 20 years: perceptions from Scottish pharmacists. Journal of Public Health, 38(4), fdv169. https://doi.org/10.1093/pubmed/fdv169
WRIGHTJR, M., VANN, R., GAMAGE, T., DAMAJ, M., & WILEY, J. (2006). Comparative effects of dextromethorphan and dextrorphan on nicotine discrimination in rats. Pharmacology Biochemistry and Behavior, 85(3), 507–513. https://doi.org/10.1016/j.pbb.2006.09.020
Wu, C. T., Yu, J. C., Yeh, C. C., Liu, S. T., Li, C. Y., Ho, S. T., & Wong, C. S. (1999). Preincisional dextromethorphan treatment decreases postoperative pain and opioid requirement after laparoscopic cholecystectomy. Anesthesia and Analgesia, 88(6), 1331–4. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/10357340
Xu, X., Zhang, B., Lu, K., Deng, J., Zhao, F., Zhao, B., & Zhao, Y. (2016). Prevention of Hippocampal Neuronal Damage and Cognitive Function Deficits in Vascular Dementia by Dextromethorphan. Molecular Neurobiology, 53(5), 3494–3502. https://doi.org/10.1007/s12035-016-9786-5
Yang, P.-P., Huang, E. Y.-K., Fu, Y.-Y., Ho, T.-S., & Tao, P.-L. (2012). Post-treatment of dextromethorphan on methamphetamine-induced drug-seeking and behavioral sensitization in rats. Synapse, 66(10), 858–869. https://doi.org/10.1002/syn.21576
Yeh, G.-C., Tao, P.-L., Chen, J. Y.-R., Lai, M.-C., Gao, F.-S., & Hu, C.-L. (2002). Dextromethorphan attenuates morphine withdrawal syndrome in neonatal rats passively exposed to morphine. European Journal of Pharmacology, 453(2–3), 197–202. https://doi.org/10.1016/S0014-2999(02)02426-3
Yoo, Y., Chung, H., Kim, E., & Kim, M. (2006). Fatal zipeprol and dextromethorphan poisonings in Korea. Journal of Analytical Toxicology, 20(3), 155–8. https://doi.org/10.1001/archpedi.160.12.1217
Yoo, Y., Chung, H., Kim, E., & Kim, M. (2017). Fatal zipeprol and dextromethorphan poisonings in Korea. Journal of Analytical Toxicology, 20(3), 155–8. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/8735195
Yu, A., & Haining, R. L. (2001). Comparative contribution to dextromethorphan metabolism by cytochrome P450 isoforms in vitro: can dextromethorphan be used as a dual probe for both CTP2D6 and CYP3A activities? Drug Metabolism and Disposition: The Biological Fate of Chemicals, 29(11), 1514–20. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/11602530
Zawertailo, L. A., Tyndale, R. F., Busto, U., & Sellers, E. M. (2010). Effect of metabolic blockade on the psychoactive effects of dextromethorphan. Human Psychopharmacology: Clinical and Experimental, 25(1), 71–79. https://doi.org/10.1002/hup.1086
Zhang, T. Y., Cho, H. J., Lee, S., Lee, J.-H., Choi, S. H., Ryu, V., … Jahng, J. W. (2007). Impairments in water maze learning of aged rats that received dextromethorphan repeatedly during adolescent period. Psychopharmacology, 191(1), 171–179. https://doi.org/10.1007/s00213-006-0548-3
Zhang, W., Qin, L., Wang, T., Wei, S.-J., Gao, H., Liu, J., … Hong, J.-S. (2005). 3-Hydroxymorphinan is neurotrophic to dopaminergic neurons and is also neuroprotective against LPS-induced neurotoxicity. The FASEB Journal, 19(3), 395–397. https://doi.org/10.1096/fj.04-1586fje
ZHANG, W., WANG, T., QIN, L., GAO, H.-M., WILSON, B., ALI, S. F., … LIU, B. (2004). Neuroprotective effect of dextromethorphan in the MPTP Parkinson’s disease model: role of NADPH oxidase. The FASEB Journal, 18(3), 589–591. https://doi.org/10.1096/fj.03-0983fje
Ziaee, V., Akbari Hamed, E., Hoshmand, A., Amini, H., Kebriaeizadeh, A., & Saman, K. (2005). Side effects of dextromethorphan abuse, a case series. Addictive Behaviors, 30(8), 1607–1613. https://doi.org/10.1016/j.addbeh.2005.02.005
Ziemann, U., Chen, R., Cohen, L. G., & Hallett, M. (1998). Dextromethorphan decreases the excitability of the human motor cortex. Neurology, 51(5), 1320–1324. https://doi.org/10.1212/WNL.51.5.1320
Currently took some dxm and doh about 30 mins ago I’m just getting to know dissociatives and I’m really interested in them but I was wondering can dxm increase the effect of other antihistamines ?