









Alprazolam is a common benzodiazepine in medical settings that is also taken for recreational purposes. It’s normally used for anxiety and panic disorder, though it has antidepressant properties.
The drug’s recreational effects include anxiolysis, disinhibition, and euphoria.
It was the top benzodiazepine in the US within a few years of its introduction. The substance has remained one of the most common psychoactive medicines.
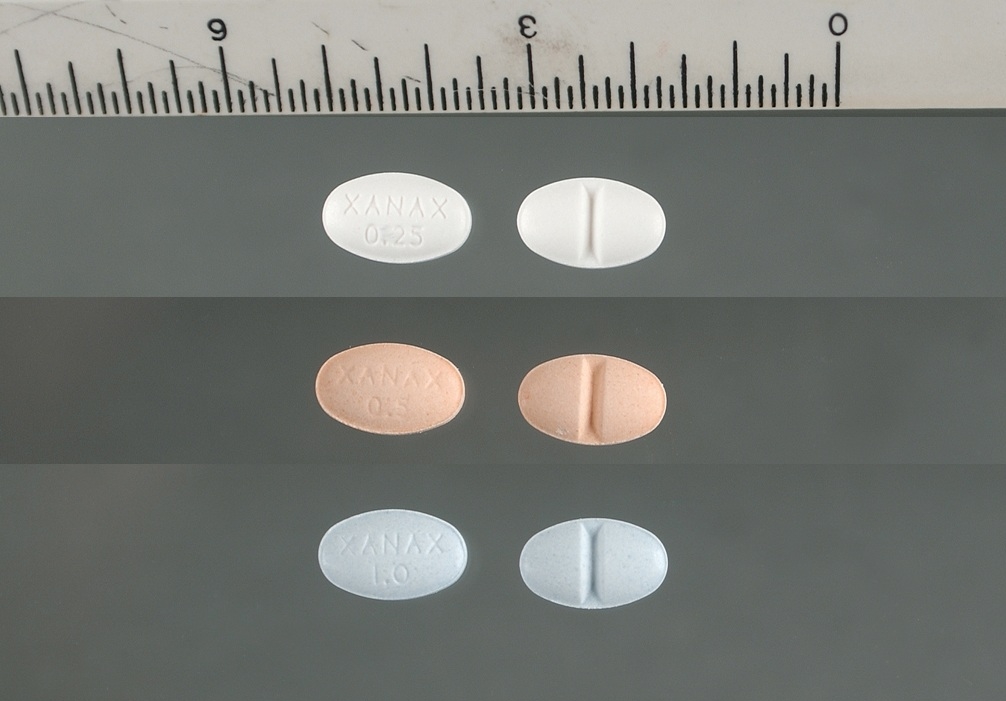
Alprazolam = Xanax; Trankimazin; Tafil; Niravam
PubChem: 2118
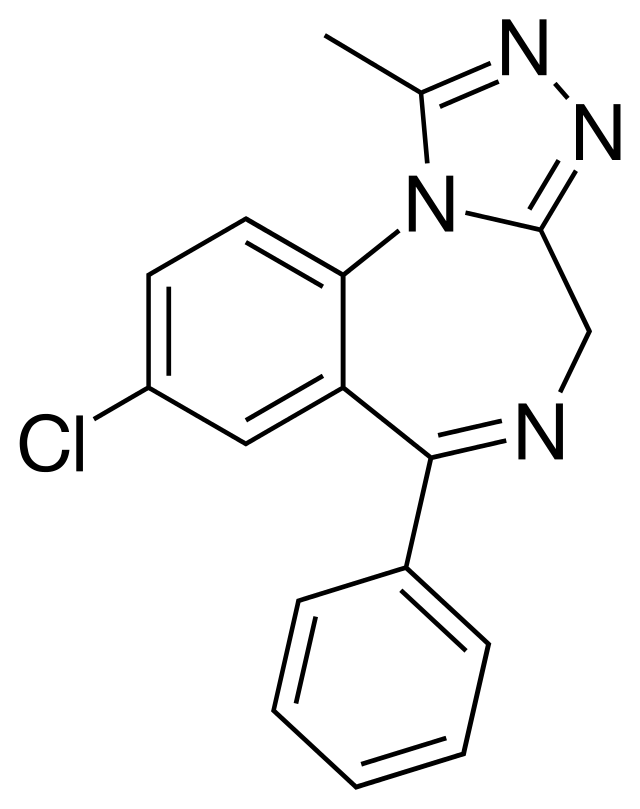
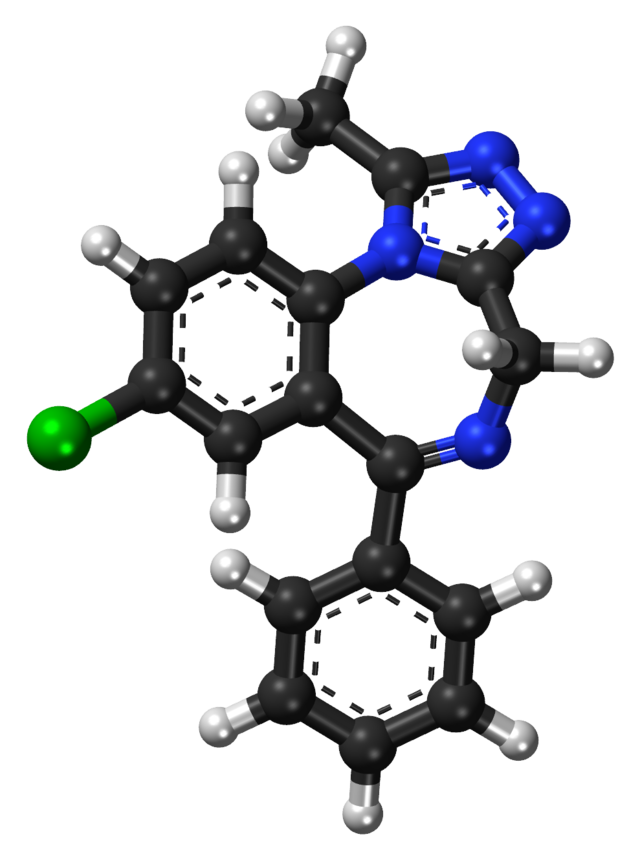
Molecular formula: C17H13ClN4
Molecular weight: 308.769 g/mol
IUPAC: 8-chloro-1-methyl-6-phenyl-4H-[1,2,4]triazolo[4,3-a][1,4]benzodiazepine
Contents
Dose
Oral
Light: 0.25 – 0.5 mg
Common: 0.5 – 1.5 mg
Strong: 1.5 – 2 mg
Oral (medical, anxiety)
Range: 0.75 – 4 mg per day
Oral (medical, panic)
Range: 2 – 6+ mg per day
Timeline
Oral
Total: 4 – 7 hours
Onset: 00:20 – 00:40
Oral (IR, medical)
Total: 3 – 6 hours
Oral (CR, medical)
Total: Over 12 hours
A lower peak plasma concentration is seen with the controlled release form, which may have the benefit of reducing the sedation.
Experience Reports




















Effects
Positive
- Anxiolysis
- Sedation
- Insomnia reduction
- Muscle relaxation
- Disinhibition
Negative
- Amnesia
- Drowsiness
- Headache
- Dry mouth
- Depression
- Confusion
The primary negative effect in medical settings is drowsiness, which declines after the first few weeks. Other negatives that aren’t as common include fatigue, slurred speech, and memory impairment.
Recreational effects
Some users find it’s very recreational, while others prefer alternative benzodiazepines. It reliably offers anxiolysis, relaxation, and sedation. Euphoria is also possible to varying degrees.
Amnesia is a real possibility with strong+ doses.
Medical efficacy
Alprazolam is mainly used as an anxiolytic and in the treatment of panic disorder, but it’s sometimes used in patients with depression as well.
The most common recommendation is to restrict its use to 2 – 4 weeks. It’s regularly used for much longer periods.
Generalized anxiety disorder (GAD)
Most studies have examined its effects over a period of 4 to 8 weeks at doses ranging from 0.5 to 3 mg.
There is evidence for it being more effective than placebo. Its efficacy is basically the same as diazepam and lorazepam.
Cognitive behavioral therapy (CBT) is often just as useful, with longer-lasting effects and a lack of physical dependence. For those who can go through CBT, it may be a better option.
Compared to buspirone
Over a period of six weeks with an average dose of 1.9 mg, it was as effective as 18.7 mg of buspirone. Alprazolam worked faster, but their ultimate efficacy was the same. This was supported in a second study.
Anxiety during alcohol withdrawal
It was able to reduce anxiety to the same degree as diazepam.
Panic disorder
The studies have usually been for under 8 weeks, with the most common result being that alprazolam is similar to other benzodiazepines. It’s as efficacious as tricyclic antidepressants (TCAs) and more effective than trazodone.
Compared to placebo
Placebo or alprazolam were given for 8 weeks. After three weeks, the alprazolam group was using an average of 6 mg per day.
The drug was clearly more effective after four weeks, but that usefulness declined by Week 8.
Compared to TCAs
A study with 1168 people compared it to imipramine, a TCA. Alprazolam worked faster, but they ended up being equally effective after eight weeks. The average dose was 5.7 mg.
Compared to non-drug therapy
Study 1
Behavioral therapy was more effective over a period of 15 weeks. Alprazolam was used at an average of 4.6 mg and didn’t significantly differ from placebo.
Study 2
It was tested in combination with exposure therapy in patients with agoraphobia. That combo was compared to alprazolam alone, exposure therapy, relaxation therapy, and placebo.
Alprazolam’s effects didn’t differ much from placebo, but they did manifest faster. Exposure therapy wasn’t enhanced by the drug.
Exposure therapy was found to be superior based on its efficacy and because alprazolam’s sedation persisted through the trial.
Meta-analysis
The review looked at alprazolam’s use in patients with agoraphobia in comparison with behavioral therapy.
While they were similar for the panic and anxiety symptoms, behavioral therapy was superior for the phobia aspect.
Compared to SSRIs
There’s some evidence that SSRIs are as effective or more effective while coming with fewer side effects and a lower dependence risk.
Longer-term efficacy
One paper suggested it could remain useful for many patients with minimal dose escalation. When participants in a 6-week trial were asked about their treatment 1.5 years later, 78% were still using alprazolam and hadn’t increased their dose.
Those patients still reported occassional panic attacks and agoraphobia.
Depression
Alprazolam might be better as an antidepressant than other benzodiazepines. It’s at least as effective as TCAs, according to some research. Other studies have found amitriptyline and imipramine are superior.
Review
A Cochrane review found it was as useful as TCAs, but it needed to be compared more with SSRIs. There were concerns about the quality of the studies involved in the review.
Even though there weren’t many short-term side effects, the potential for dependence could tilt the scales in favor of other antidepressants.
PTSD
A study found it could reduce general anxiety symptoms but wasn’t useful for PTSD overall.
Impairment
Alprazolam is impairing when taken acutely. Using it over long periods is at least partially protective against the impairment.
In a group of studies using 0.25 to 2 mg acutely, doses over 0.5 mg led to psychomotor impairment (increased reaction time.)
It may be most problematic when trying to maintain your performance for over 30 minutes, such as with extended highway driving. One test found 0.5 mg impaired performance on a 60-minute vigilance test. 0.8 mg impaired speed and accuracy on a 20-minute vigilance test performed 3.5-hours after administration.
Driving ability
20 healthy volunteers were given 1 mg. They then had to complete an on-road driving test, during which they were instructed to maintain a steady position for 100 km at 60 mph.
Their performance was severely impaired, leading to greater side-to-side weaving and excursions out of lane. Impairment in the Standard Deviation of Lateral Position (SDLP) test was similar to 0.15% BAC.
Of the 20, 6 had to stop the test due to falling asleep behind the wheel.
Memory effects
There is a dose-dependent impairment of acquisition and retrieval of newly learned information. Long-term memory isn’t notably impaired at common doses.
Immediate and delayed recall and recognition are impaired over 0.5 mg.
Tolerance
Just as sedation declines with use, impairment appears susceptible to tolerance. After 1-3 weeks of daily use, some research indicates there is no longer a negative effect from the drug on most tests.
In one study, delayed recall was impaired after 3 and 10 days of treatment. The impairment went away by 24 days.
Paradoxical reactions
Effects like agitation and aggression are known to occur in a small set of users. Paradoxical reactions are more common in those with preexisting aggression and psychiatric conditions like bipolar disorder. Concomitant alcohol use may raise the chance of these effects.
Here’s an example:
Case
14-year-old male had excessive anger, irritability, and was assaulting people. He said he wanted to die and planned to commit suicide by cutting himself.
This behavior began 10 days into his alprazolam treatment (1 mg/day) for anxiety. There were no other disorders and no other medication was involved.
All of this resolved after he was switched to sertraline.
Chemistry & Pharmacology
Chemistry
Alprazolam differs from many other benzodiazepines in that it contains a triazole ring. This makes it a triazolobenzodiazepine.
Pharmacology
Pharmacodynamics
It’s a GABAa positive allosteric modulator. The substance binds nonselectively to the benzodiazepine receptor on the GABAa receptor complex.
Complexes affected by the drug include the a1 subunit (sedation/amnesia) and the a2 subunit (anxiolysis).
By operating on the complex, it facilitates greater GABA binding and activity. This leads to inhibition around the brain.
Decreased cerebral blood flow can be seen.
Alprazolam is associated with greater extracellular dopamine in the striatum, something that might differ from some benzodiazepines.
Pharmacokinetics
Peak plasma concentration: 12 – 22 ug/L (single 1 mg dose)
Tmax (oral): 1 – 2 hours
Tmax (sublingual): 2.8 hours
Tmax (IV): 30 minutes
Half-life: 9 – 16 hours
Bioavailability (oral): 90%
The drug easily crosses the blood-brain barrier.
Metabolism
It is primarily metabolized in the liver by CYP3A4. There are at least 29 metabolites, of which 4-hydroxy-alprazolam and a-hydroxy-alprazolam are the primary ones.
Both of those metabolites are present at low concentrations and have a lower BZ affinity. They don’t really contribute to the pharmacology.
80% of alprazolam is excreted unchanged by the kidneys.
History
1969
The patent for alprazolam was filed by Upjohn.
1970s
While research on the drug was taking place, other benzodiazepines were already on the market and growing in popularity.
Animal research showed it was more potent than diazepam and offered anxiolytic effects.
1981
Following human trials which further demonstrated its anxiolytic activity, alprazolam was released by Upjohn as “Xanax.”
It was the first triazolobenzodiazepine to be approved for anxiety.
1980s – 1990s
Studies and case reports showed the substance could be useful in panic disorder and other conditions. It also became clear that physical dependence occurs in medical settings following weeks of use.
There was interest in using it for adolescent anxiety.
1985 – 1988
Emergency room admissions involving the drug increased by 50%.
Alprazolam was the top benzodiazepine in the US and one of the top prescriptions overall by 1988.
1991
Approved in the US for panic disorder.
1990s
There was a rise in its use for panic disorder, despite there being first-line treatments, like SSRIs.
1997 – 2007
Prescriptions for alprazolam increased 71% in the US. They increased 99% in Australia.
2014
Australia rescheduled it to Schedule 8 due to a rise in illicit use and concerns about its relative toxicity and misuse potential.
2016
It’s the most prescribed benzodiazepine in the US and one of the most popular in recreational settings.
Legal Status
USA
Schedule 4
Controlled
It is illegal in many other countries when not prescribed. You should check your local laws to verify its legal status.
Among the countries that treat it as a controlled drug are Australia, Canada, and the UK.
Safety
Most of the deaths and near-fatal cases have involved polydrug use. Taking it with other depressants, which is quite common, is particularly dangerous.
There’s been some suggestion that it may be more toxic than other benzodiazepines. Even when other factors are corrected for, alprazolam is associated with an increase in the following:
- Length of hospital stay
- Likelihood of mechanical ventilation
- Flumazenil administration
- ICU admission
Pregnancy
It appears to raise the chance of congenital abnormalities during the first trimester. It can be detected in breast milk.
Acute safety issues
The primary acute concerns are amnesia and cognitive impairment. Severe overdoses could lead to respiratory depression and coma. It’s far more dangerous when combined with other depressants.
Many people attempt suicide each year using alprazolam, but the vast majority are unsuccessful.
Here’s an example of a near-fatal case:
Case 1
- 15-year-old male
- Alprazolam and heroin detected
- Found unresponsive, required intubation for over a day
Deaths
It’s unusual for alprazolam alone to be found in a drug overdose death. Other depressants are normally involved.
Here are some case reports:
Case 1
- 30-year-old female
- Found dead with tramadol, alprazolam, and wine near her
- Blood concentration: 0.21 mg/L
Case 2
- 44-year-old female
- Found dead in bed–she had a history of psychiatric problems
- She was prescribed alprazolam, fluoxetine, phenytoin, lorazepam, and venlafaxine
- Heart blood: 2.1 mg/L
Case 3
- Depressed and suicidal female
- Blood: 0.177 mg/L
Case 4
- Alprazolam and ethanol
- Blood: 0.122 mg/L
Tolerance & Withdrawal
Tolerance
Tolerance builds over time and is associated with lower GABAa benzodiazepine receptor density. In one study, receptor density was lower after 24 days of 2 mg daily.
Withdrawal
Withdrawal includes insomnia, anxiety, agitation, depression, restlessness, seizures, and delirium. It reliably occurs afters weeks of use, with the severity affected by your daily dose and how long it’s been used.
Tapering over a period of weeks or months is recommended. During this time, withdrawal may still appear, but it’s usually less severe. Tapering reduces the chance of rebound anxiety. Alprazolam does lose its effectiveness as the dose is reduced.
Research has found 4-week tapers still result in rebound anxiety/panic in 25-30% of patients. Combining the drug with CBT may reduce the withdrawal and rebound symptoms.
Here are some case reports:
Case 1
A woman used it for 8 weeks, rising from 1 mg to 6 mg daily. This was then reduced by 1 mg every 3 days.
A headache developed on the 12th day of dose reduction. The patient’s final 1 mg dose was taken on Day 13.
On Day 14, she had a severe headache and a tonic-clonic seizure.
Case 2
68-year-old man with depression became delirious after two days without his alprazolam. He had been taking 1.5 mg per day.
Diazepam and haloperidol were ineffective in alleviating the delirium. Alprazolam re-administration was effective.
Case 3
43-year-old female had been on diazepam for years. Alprazolam replaced the diazepam 10 days prior to admission.
She was told to use 2 mg (3x daily), but she ended up using ~200 mg over the course of six days.
Four days after running out, she experienced severe insomnia. She took 60 mg of zolpidem to overcome the insomnia, yet she developed hallucinations instead and presented in the emergency department (ED).
She was hypertensive, hyperthermic, and tachycardic (130). She was suffering from shaking episodes.
14 hours after admission to the ED, she was found dead. Initially it was believed to be a zolpidem overdose, but the final conclusion was that alprazolam withdrawal caused the death.
Risky Combos
Other depressants, including ethanol, opioids, and benzodiazepines.
Alcohol at moderate doses has been found to cause additive (not synergistic) impairment. Higher doses of alcohol cause synergistic impairment. The combination may also increase aggression and irritability.
References
(2016) Motivational drive and alprazolam misuse: A recipe for aggression?
(2015) Use of alprazolam for treatment of essential tremor
(2015) Alprazolam Dependence – The Sting in the Tail: A Case Report
(2015) Management of benzodiazepine misuse and dependence
(2015) Paradoxical reactions related to alprazolam.
(2015) Temporal profile of brain response to alprazolam in patients with generalized anxiety disorder.
(2014) Circumstances and toxicology of sudden or unnatural deaths involving alprazolam
(2013) Alprazolam dependence: A case report
(2013) Benzodiazepine Pharmacology and Central Nervous System–Mediated Effects
(2012) The role of alprazolam for the treatment of panic disorder in Australia.
(2012) Characteristics of alprazolam-related deaths compiled by a centralized state medical examiner.
(2012) Alprazolam as a suicidal drug-a new trend
(2012) Alprazolam for depression
(2011) Efficacy of alprazolam sublingual tablets in the treatment of the acute phase of panic disorders.
(2005) Acute effects of alprazolam on risky decision making in humans.
(2005) Alprazolam-related deaths in Palm Beach County.
(2004) Alprazolam is relatively more toxic than other benzodiazepines in overdose
(2004) The acute effects of L-theanine in comparison with alprazolam on anticipatory anxiety in humans.
(1999) Fatal overdose of tramadol and alprazolam
(1997) A fatality due to alprazolam intoxication.
(1994) Pharmacologic effects and abuse liability of bretazenil, diazepam, and alprazolam in humans.
(1993) Abuse liability of alprazolam relative to other commonly used benzodiazepines: a review.
(1993) Alprazolam in panic disorder: a retrospective analysis.
(1993) Clinical pharmacokinetics of alprazolam. Therapeutic implications.
(1991) History of benzodiazepine dependence.
(1991) Alprazolam versus buspirone in the treatment of outpatients with generalized anxiety disorder.
(1991) Alprazolam and diazepam: addiction potential.
(1990) Alprazolam use and dependence. A retrospective analysis of 30 cases of withdrawal.
(1987) Pharmacology of the benzodiazepines; with special emphasis on alprazolam.
(1986) Alprazolam-induced manic episode in two patients with panic disorder.
(1986) Seizures Following the Withdrawal of Alprazolam
(1986) Withdrawal syndrome with gradual tapering of alprazolam.
(1985) Alprazolam withdrawal delirium unresponsive to diazepam: case report.
(1985) Alprazolam: Review of pharmacological, pharmacokinetic, and clinical data
(1984) Emergence of hostility during alprazolam treatment.
(1984) Pharmacokinetics and pharmacodynamics of alprazolam after oral and IV administration.
(1982) Alprazolam: pharmacokinetics, clinical efficacy, and mechanism of action.







